

Volume 16, Issue 3 (May & June 2025)
BCN 2025, 16(3): 657-666 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Salari Zare M, Mir M, Shobeiri S S, Tehrani H, Amiri P, Aldaghi M A et al . Determining Pro-oxidant Antioxidant Balance in Febrile Children With and Without Seizure: A Comparative Study. BCN 2025; 16 (3) :657-666
URL: http://bcn.iums.ac.ir/article-1-2942-en.html
URL: http://bcn.iums.ac.ir/article-1-2942-en.html
Mohammad Salari Zare1 

 , Mehran Mir2 , Saeideh Sadat Shobeiri3 , Houman Tehrani2 , Parastoo Amiri4 , Mitra Azra Aldaghi2 , Kazem Hassanpour *2
, Mehran Mir2 , Saeideh Sadat Shobeiri3 , Houman Tehrani2 , Parastoo Amiri4 , Mitra Azra Aldaghi2 , Kazem Hassanpour *2
, Mehran Mir2 , Saeideh Sadat Shobeiri3 , Houman Tehrani2 , Parastoo Amiri4 , Mitra Azra Aldaghi2 , Kazem Hassanpour *2
1- Department of Neurology, School of Medicine, Sabzevar University of Medical Sciences, Sabzevar, Iran..
2- Department of Pediatrics, School of Medicine, Sabzevar University of Medical Sciences, Sabzevar, Iran.
3- Cellular and Molecular Research Center, Sabzevar University of Medical Sciences, Sabzevar, Iran.
4- Iranian Research Center on Healthy Aging, Sabzevar University of Medical Sciences, Sabzevar, Iran.
2- Department of Pediatrics, School of Medicine, Sabzevar University of Medical Sciences, Sabzevar, Iran.
3- Cellular and Molecular Research Center, Sabzevar University of Medical Sciences, Sabzevar, Iran.
4- Iranian Research Center on Healthy Aging, Sabzevar University of Medical Sciences, Sabzevar, Iran.
Full-Text [PDF 610 kb]
| Abstract (HTML)
Full-Text:
1. Introduction
Febrile seizure (FS) is a benignant circumstance that occurs between six and sixty months of age with a temperature of 38 °C or more, which is not a result of central nervous system (CNS) infection or metabolic imbalance and has no history of previous seizures (Bakhtiari et al., 2023). FS is the most common type of seizure in children, with a prevalence of 2–5% (Delpisheh et al., 2014; Rivas-García et al., 2022). Risk factors for FS include premature birth, brain disorders, and family history (Bakhtiari et al., 2023; Sharawat et al., 2016). There are two types of FSs: Simple and complex. A simple FS is an initial generalized seizure, typically tonic-clonic, accompanied by fever, that lasts <15 minutes and does not recur within 24 hours. Complex FSs last at least 15 minutes, are accompanied by focal neurologic symptoms, or reoccur within 24 h (Smith et al., 2019). Various factors contribute to the recurrence of attacks, including age, sex, family and personal history of seizures, body temperature at the time of seizure, and the interval between the onset of fever and seizure (Talebian & Mohammadi, 2009).
Reactive oxygen species (ROS) are a family of unstable molecules composed of oxygen and one or more unpaired electrons in the outermost shell. ROS are highly reactive compounds due to the presence of unpaired electrons (León Navarro et al., 2020). The most prevalent ROS are hydroxyl radicals, superoxide anions, and hydrogen peroxide. In a healthy body, these radicals play a crucial role in cellular communication, development, apoptosis, and systemic functions, such as blood pressure regulation and immunological responses (Brieger et al., 2012; León Navarro et al., 2020). Conversely, oxidative stress occurs when the body produces more ROS than the antioxidant defense system can eliminate. Under these circumstances, basic cell macromolecules, including DNA, lipids, and proteins, can be oxidized (León Navarro et al., 2020). Crucial enzymes may alter both structure and function as a result of protein oxidation (Stadtman, 2001). Lipid peroxidation can change the fluidity, permeability, and protein-membrane functions, leading to hyperexcitability (Wong-Ekkabut et al., 2007). An imbalance between the production of ROS and the antioxidants that scavenge them causes oxidative stress (León Navarro et al., 2020).
Recent research has demonstrated the involvement of lipid peroxidation and free oxygen radicals in the pathophysiology of several diseases. Numerous diseases, including asthma, diabetes mellitus; rheumatologic conditions, such as rheumatoid arthritis and cancer; neurological conditions, including stroke and epilepsy; and inflammatory disorders have all been linked to oxidative stress (Kumar & Kumari, 2017; Leung et al., 2018). The production of lipid peroxidation and free radicals accelerates cell death (Bakhtiari et al., 2023). The body develops defense systems to stop oxidants, such as free radicals and lipid peroxidation, from causing damage. These are the “antioxidant defense systems,” which include glutathione reductase (GR), glutathione peroxidase (GPx), superoxide dismutase (SOD), and catalase (CAT) (Bakhtiari et al., 2023; Fetveit, 2008; Vidailhet et al., 2017) A disturbance in the equilibrium of pro-oxidant antioxidants is commonly referred to oxidative stress, and it plays a role in the development of multiple neurodegenerative diseases, autoimmune disorders, and cancer (Avval et al., 2018). In this regard, the present study aimed to evaluate the pro-oxidant-antioxidant balance (PAB) in febrile children with and without seizures.
2. Materials and Methods
This cross-sectional study was conducted at Heshmatieh Hospital, Sabzevar University of Medical Sciences, Sabzevar, Iran, between March 2020 and March 2021.
Eighty children, aged six months to five years, were selected from among patients admitted to Heshmatieh Hospital in Sabzevar using non-random sampling. Forty febrile children with a temperature of 38 °C and above (F) and 40 febrile children who had experienced their first FS were included. Blood samples were collected from each patient. In the case of patients with fever and seizures, the serum sample was taken in the second hour after the seizure, that is, between one and two hours after the seizure, and in the case of patients with fever and without seizures, the blood sample was taken when the fever was 38 degrees or higher. Patients with seizures without fever and a history of seizures without fever in the past, those suffering from developmental disorders and cerebral palsy, those suffering from metabolic and genetic diseases, and those with syndromes that cause or accompany seizures were excluded. The patient serum samples were prepared and stored at -20 °C until the PAB test was performed.
The PAB test
The PAB test, is a method that simultaneously determines the oxidants and antioxidants of the target sample in a single test (Alamdari et al., 2007). The PAB measurement method in our study involved investigating the activity of both oxidants and antioxidants simultaneously, tetramethylbenzoyl (TMB) was used as an oxidation-reduction index due to its electrochemical and optical properties to evaluate PAB (Boskabadi et al., 2022). The pro-oxidant-antioxidant ratio values were expressed in HK (HK unit, H: Hamidi Alamdari, K: George Koliakos) (Boskabadi et al., 2022). HK is an optional unit that is calculated based on the percentage of hydrogen peroxide absorbed in the standard solution (Samani et al., 2022). An improved PAB was used according to a previously described method (Avval et al., 2018; Boskabadi et al., 2022; Tavana et al., 2016). Briefly, a standard curve was drawn using 0%-100% ratios of 250 μM hydrogen peroxide with 3 μM uric acid (in 10 mM sodium hydroxide). Based on the concentration of hydrogen peroxide in the reaction, the peroxidase enzyme oxidizes the TMB substrate, which is observed as a blue color. At the end of the reaction, hydrochloric acid produced a yellow color at a wavelength of 450 nm. The absorbance was measured at 450 nm with a reference wavelength of 620 nm using an ELISA reader. Finally, pro-oxidant-antioxidant ratio values were expressed in HK units.
Statistical analysis
In the description of the data, appropriate statistical tables and indices, such as Mean±SD, etc. were used. In the analysis of the data, the normality of the data was first investigated using the Shapiro-Wilk test, which confirmed normality. For normal data, appropriate parametric methods, such as student’s t-test, were used. In cases of non-normality, Mann-Whitney and Wilcoxon’s tests were used. The Pearson chi-square test was used for data analysis with nominal scales, and in cases where more than 20% of the expected frequencies in the tables were less than 5 (Cochran), Fisher’s exact test was used. IBM-SPSS software, version 20 was used for the analysis.
3. Results
In this study, 80 patients, including 32 girls (40%) and 48 boys (60%), with a mean age of 36.67±18.12 months and an age range of 6-60 months. HK and fever variables were evaluated in the FS (fever and seizures) and F (fever) groups. The variables of duration of fever, duration of seizures, type of seizures, frequency of seizures, history of seizures, history of epilepsy in first-degree relatives of the patient, history of epilepsy in other relatives of the patient, history of fever and seizures in first-degree relatives of the patient, and history of fever and seizures in other relatives were examined only in the FS group patients.
The age range (maximum and minimum) in both groups was 6 to 60 months. The Mean±SD of age in the FS and F groups was 35.63±18.20 months and 37.73±18.21 months, respectively, and no significant difference was observed between the two groups in terms of age (P=0.567). The number of girls in each of the FS and F groups was 16(40%). The number of boys in each of the FS and F groups was 24(60%). The gender distribution in the studied groups did not differ significantly from one another (P=1.00). Therefore, the two groups were similar in terms of age and sex.
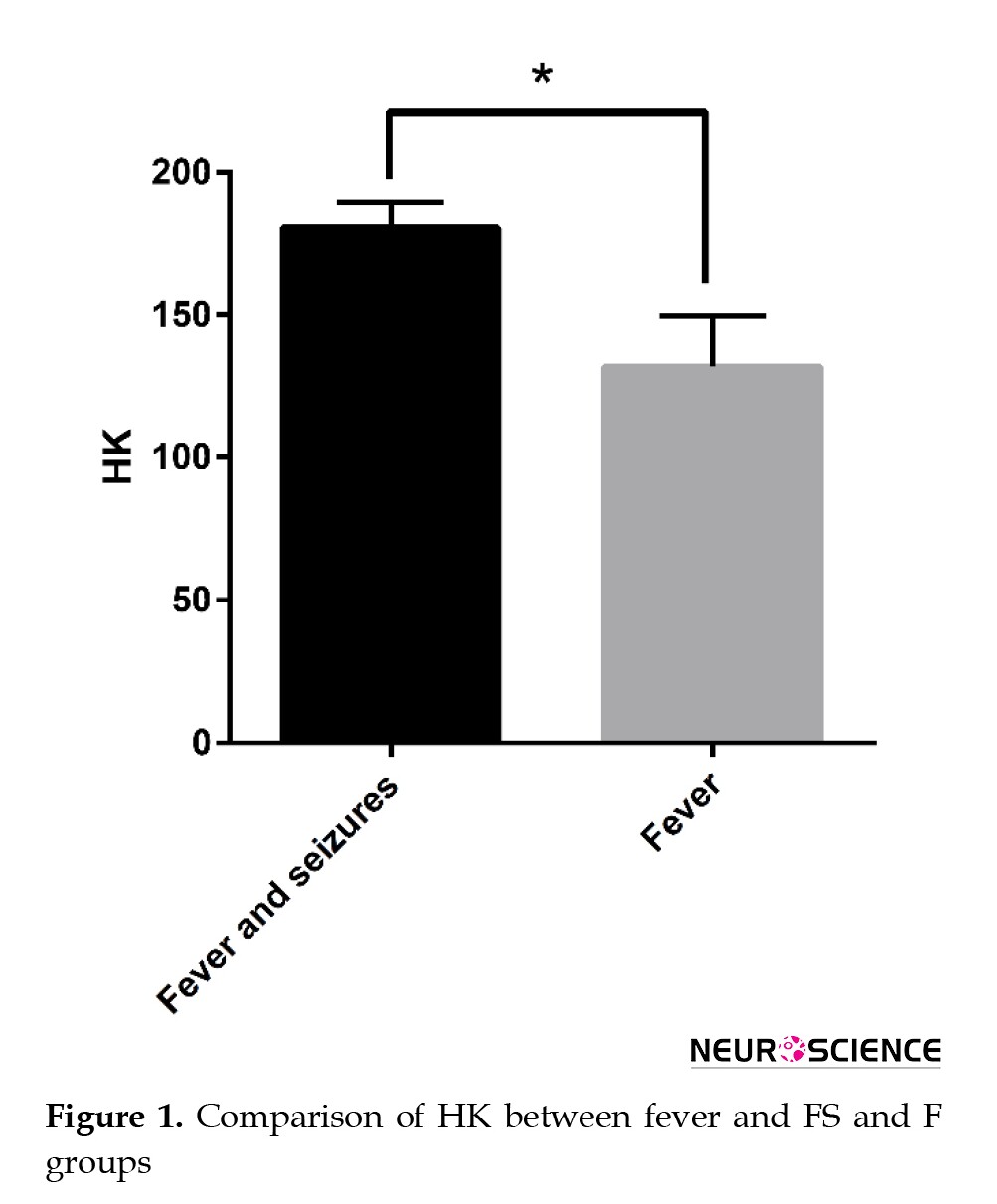
Comparison of HK between FS and F groups
The range of observed HK (the difference between the highest and lowest HK) was 43.54 in the FS group and 66.93 in the F group. The Mean±SD of HK in the FS group was 180.43±9.28, and in the F group was 131.83±17.73. In terms of the average HK, the two groups were significantly different from each other (P<0.001), and the F group had lower HK compared to the FS group (Figure 1).
Comparison of fever between groups
According to the patients’ results, the number of patients with a fever of 38-39 °C was 28(70%) in the FS group and 29(72.5%) in the F group. The number of patients with a fever of >39 °C in the FS and the F groups was 12(30%) and 11(27.5%), respectively. The distribution of patients with varying degrees of fever among the studied groups did not significantly differ from one another (P=0.805).
Comparison of HK between groups of fever degrees according to FS and F groups
In the FS group, the mean HK in the group with a fever of 38-39 °C was lower than the group with a fever over 39 °C, but the difference was not significant (P=0.095). In the F group, the average HK was higher in the group with a fever of 38-39 °C than in the group with a fever >39 °C, but the difference was not significant (P=0.083).
Relationship between age and HK variables
In the FS group, age had an inverse relationship with HK, but the correlation value was not significant (r=-0.032, P=0.845). In the F group, age had a direct relationship with HK; however, the correlation value was not significant (r=0.102, P=0.529).
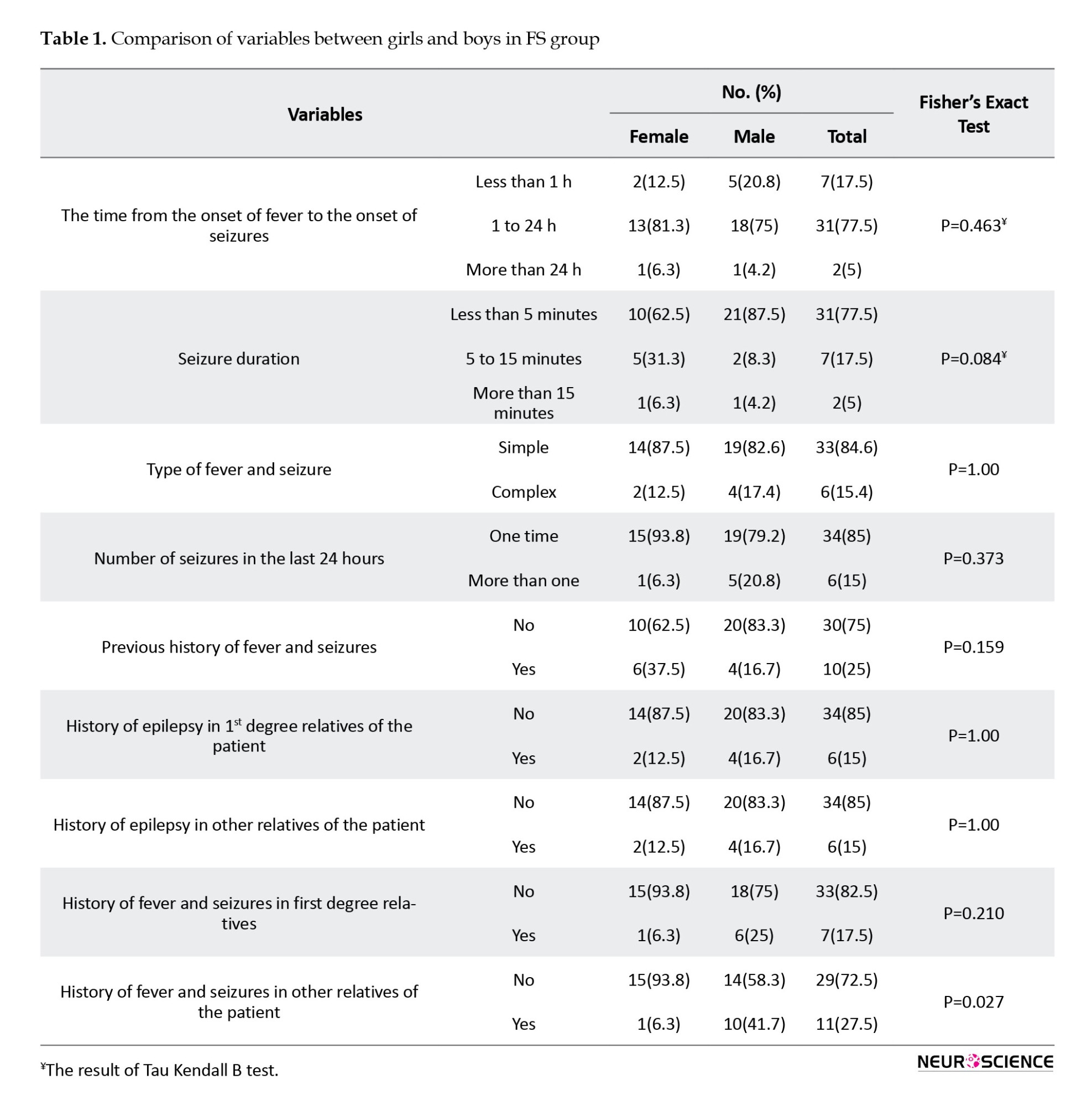
Comparison of variables between girls and boys in FS group
The frequency distribution of fever and seizures in other relatives of male patients was significantly higher than that in female patients (P=0.027). No significant differences were observed between girls and boys in the frequency distribution of the other variables (Table 1).
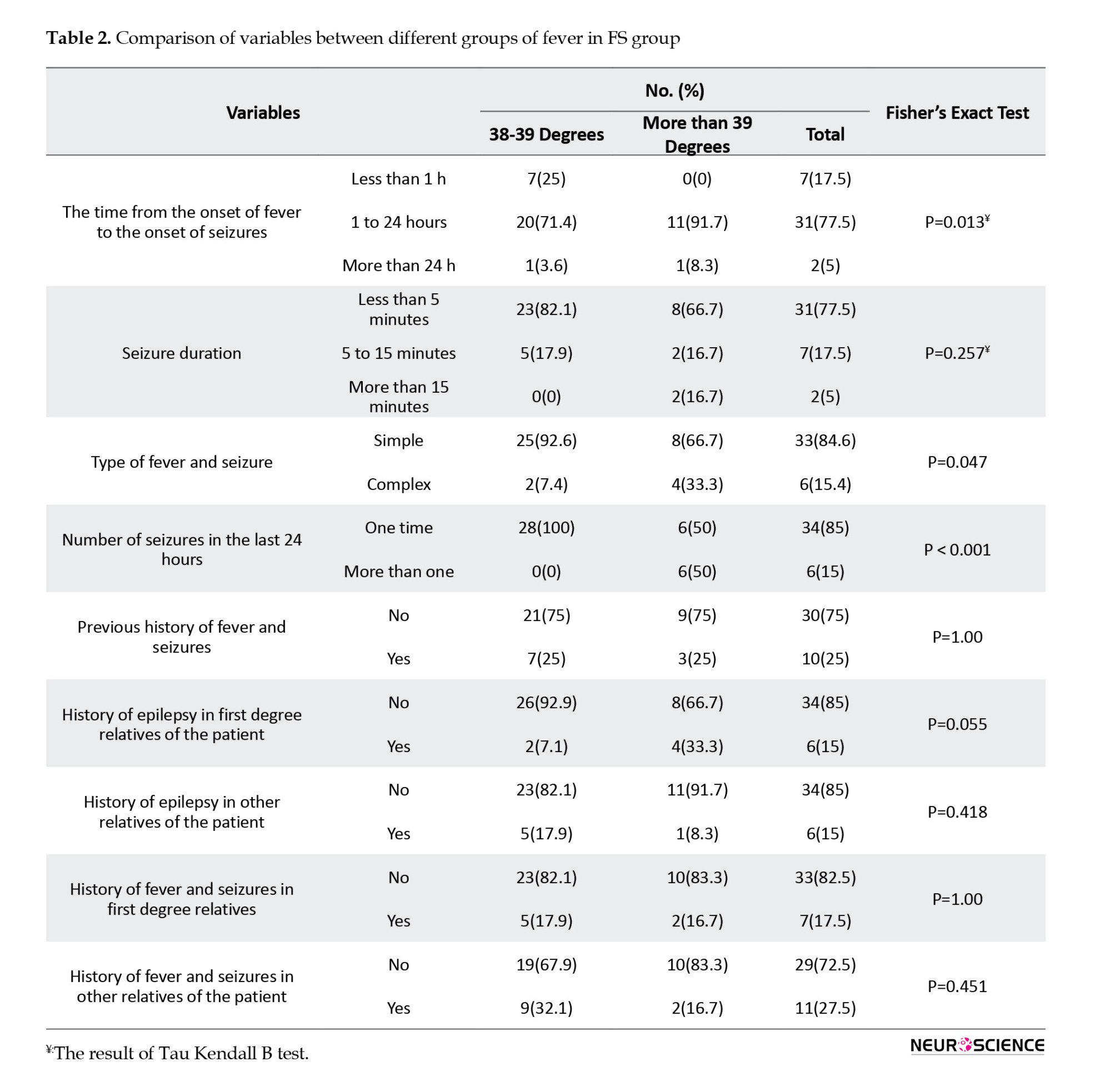
Comparison of variables between different groups of fever in FS group
The frequency distribution of the time from the onset of fever to the onset of seizures was significantly different between patients in the group with a temperature of >39 °C and the group with a temperature of 38-39 °C (P=0.013). The frequency distribution of fever and complex seizures was significantly higher in the >39 °C group than in the 38-39 °C (P=0.047). The distribution of the frequency of fever and seizures in 24 h was significantly higher in the 39 °C group than in the 38-39 °C (P<0.001). No significant difference was observed in the frequency distribution of other variables between patients in the group with a temperature of >39 °C and the group with a temperature of 38-39 °C (Table 2).
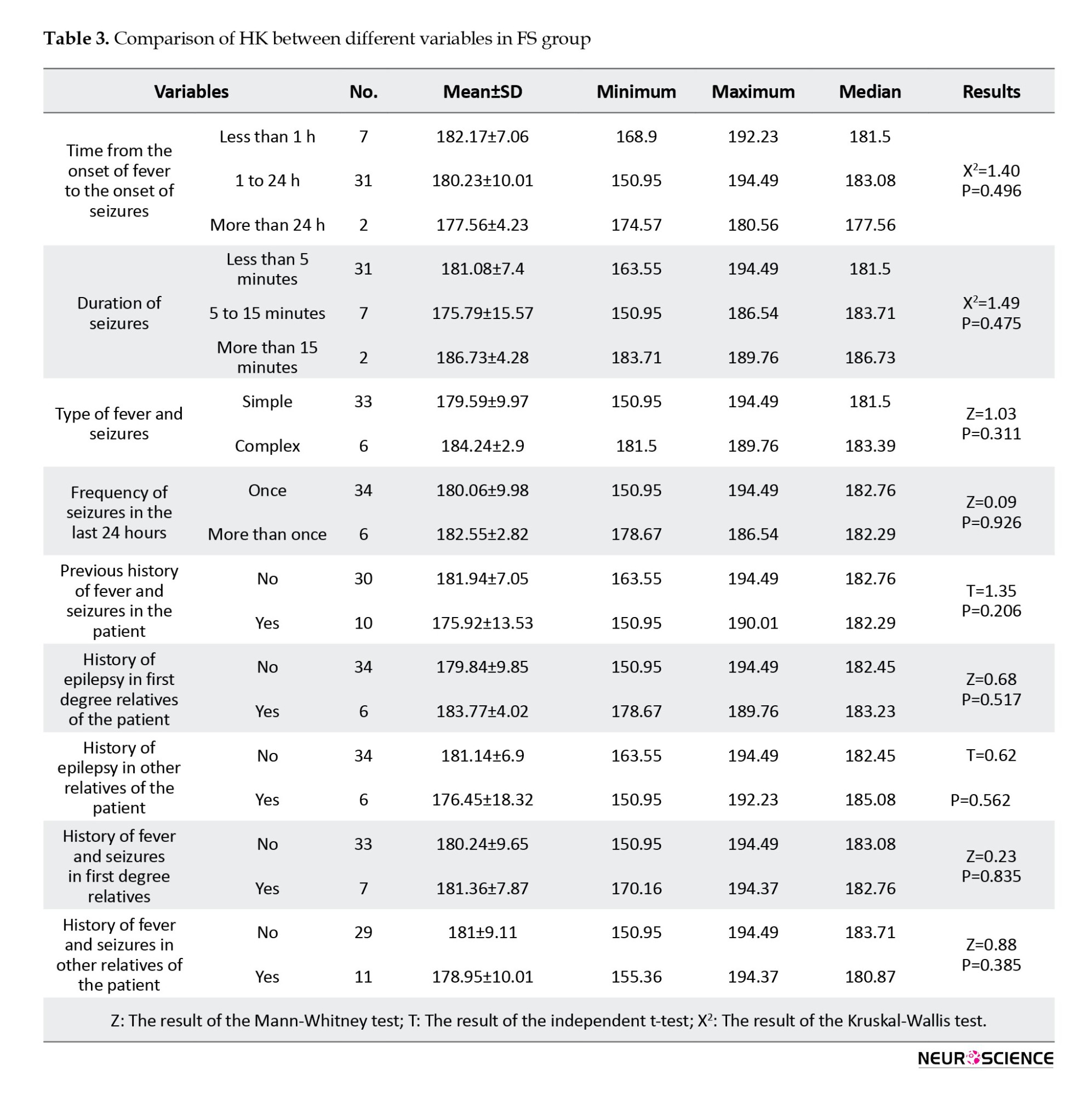
HK comparison between different variables in FS group
In the FS group, the average HK between the levels of any of the variables of time from the onset of fever to the onset of seizures, duration of seizures, type of fever and seizures, frequency of seizures in the last 24 h, previous history of fever and seizures in the patient, history of epilepsy in first-degree relatives of the patient, history of epilepsy in other relatives of the patient, history of fever and seizures in first-degree relatives, and history of fever and seizures in other relatives of the patient showed no significant difference (P<0.05) (Table 3).
4. Discussion
In this study, 80 patients, including 32 girls (40%) and 48 boys (60%), with a mean age of 36.67±18.12 months and an age range of 6 to 60 months in the groups of febrile patients with and without seizures, were evaluated in terms of HK variables and degree of fever.
In our study, the average age was 36.67±18.12 months, with an age range of 6 to 60 months. Also, the age range (maximum and minimum age) in both groups was 6-60 months. The Mean±SD of age in the FS and F group was 35.63±18.20 months and 37.73±18.21 months, respectively, and no significant difference was observed between the two groups in terms of age. In the study by Iyshwarya et al. (2013), the average age of children with fever and seizures was 3.05±2.19 years; in those with only fever, it was 3.11±1.24 years; and in the control group, it was 3.86±1.18. In the study by Abuhandan et al., the average age was 26.65±12.58 months for the group with fever and seizures and 11.53±30.46 months for the control group. In this study, no statistically significant difference was observed between the two groups in terms of age (Abuhandan et al., 2013). In another study, the average age of patients with fever and seizures was 2.13±0.82 years. In the group of febrile children without seizures, serving as a control, the average age was 2.47±1.16 years, with no significant difference in terms of age (El-Masry et al., 2018).
Our results showed that the number of girls in each of the FS and F groups was 16(40%). The number of boys in each of the FS and F groups was 24(60%). The gender distribution in the studied groups did not differ significantly from one another. In a study by Iyshwarya et al., no significant gender differences were observed in children with fever and seizures (Iyshwarya et al., 2013). In a cross-sectional study conducted in Iran, no significant gender difference was observed regarding FSs in children aged 6 months to 5 years (Ehsanipour et al., 2009). However, Mollah et al. (2008) revealed that male children were more prone to fever and seizures than female children.
In the current study, of 40 patients with fever and seizures (FS group), 34 had simple fever and seizures (85%), and 6 had complex fever and seizures (15%). Similar to our findings, a study by Gϋnes et al. reported that of 31 patients in the fever and seizure group, 25 patients (80%) had simple FSs, and six patients (20%) had complex FSs (Güneş et al., 2009).
FSs are defined as seizures between six and sixty months of age with a temperature of 38 °C or more, which is not a result of CNS infection or metabolic imbalance, and have no history of previous FSs. Many studies have considered factors, such as fever background, seizures in first-degree relatives, micronutrient deficiency, immunological reactions, and oxidative stress as potential aggravating factors (Hartfield, 2010; Pacitti et al., 2013). Seizures are the most common cause of emergency department visits and hospitalizations in children (Salmi et al., 2021). Children with early-onset fever and seizures, especially those with recurrent fever and seizures, may be at greater risk of poorer verbal and processing performance and are therefore at risk of cognitive and functional impairments (Billstedt et al., 2020). A complex interaction among the brain, genetics, epigenetics, and early environment is involved in fever and seizures (Mewasingh et al., 2020). Fever and convulsions are considered responses of the developing brain to fever, but their exact pathophysiology remains unknown. A set of environmental and genetic factors are involved in its creation. Specific mutations in ion channels make individuals susceptible to fever and seizures. Oxidative stress disturbance of the balance between antioxidants and pro-oxidants in the body (Momen Beitollahi et al., 2010). Antioxidants eliminate free radicals in the body. In contrast, compounds that can produce oxygen-free radicals in the body are called pro-oxidants (Kunz, 2002). Some types of free radicals contain nitrogen, while others are produced during harmful processes and contain oxygen, which, upon formation, damages proteins, lipids, and DNA (Momen Beitollahi et al., 2010). In contrast, seizures lead to the production of free radicals. Therefore, oxidative stress and the production of free radicals are currently recognized as key effects of seizures (Valko et al., 2007). Recent data have shown that disorders in the antioxidant system make the nervous system vulnerable and increase a person’s susceptibility to convulsive attacks (Martinc et al., 2012). In other words, free radical production provokes convulsive attacks (Laus et al., 2017).
In this study, pro-oxidant-antioxidant ratio values were expressed in HK units. This optional unit is calculated based on the percentage of hydrogen peroxide absorbed in the standard solution. The Mean±SD of HK in the FS group was 180.43±9.28, and in the F group, it was 131.83±17.73. The two groups were significantly different in terms of the other (P<0.001). Therefore, the amount of HK in patients in the FS group was significantly higher than in patients in the F group, and this proved that the amount of oxidative stress in patients with fever and seizures is higher than in patients with fever but without seizures. The PAB in the FS group was disturbed compared to the F group.
Compared to previous studies, no similar study was found that measured and compared the PAB of serum samples from patients with fever and seizures versus those with fever without seizures using the PAB test. However, in other studies, the levels of antioxidants and the amount of oxidative stress have been measured and compared in patients with fever and seizures, as well as in patients with fever, using other methods. Akarsu et al. measured the levels of erythrocyte arginase, plasma malondialdehyde (MDA), erythrocyte CAT, cerebrospinal fluid MDA, cerebrospinal fluid nitric oxide, and plasma nitric oxide. Their results indicated that the level of free radicals was significantly higher in the FS group than in the control group. Also, the authors showed that the risk of free radicals in seizures without fever was significantly higher than in seizures with fever (Akarsu et al., 2007). In the study by Gϋnes et al., erythrocyte MDA and GPx levels were significantly higher. In contrast, SOD levels were significantly lower, in the group of patients with fever and seizures. This result, consistent with our study’s results, showed a direct relationship between the occurrence of seizures caused by fever and increased levels of free radicals (Güneş et al., 2009). Increased MDA levels indicate the loss of fatty acids, leading to cell membrane damage and cell death. Akarsu et al. investigated the effects of fever and FSs on the oxidant status in children finding that the plasma MDA level was increased in children who had FSs (Akarsu et al., 2007). Moreover, the enzymes SOD and GPx play protective roles against free radicals. Gϋnes et al. showed that SOD levels decreased and GPx levels increased after FSs. Overproduction of superoxide may occur in fever and seizures, and decreased levels of SOD may result in reduced catalysis of superoxide to oxygen and hydrogen peroxide. GPx activity may enhance the conversion of hydrogen peroxide to water as a compensatory mechanism (Güneş et al., 2009). Although it is well-known that seizures cause oxidative stress, the effects of fever and seizures on oxidative balance remain unclear (Akarsu et al., 2007). In Iyshwarya et al.’s study, the increase in the stress marker MDA among children with fever and seizures and the decrease in serum levels of zinc and magnesium as antioxidants in this group, indicated that oxidative stress had increased among those with fever and seizures (Iyshwarya et al., 2013).
In conjunction with our study, Abu-Handan et al. showed that oxidative stress is higher in patients with fever and simple seizures than in healthy individuals, and that it plays a crucial role in the occurrence of FSs (Abuhandan et al., 2013).
5. Conclusion
According to our results, the average serum level of PAB in febrile children with seizures was significantly higher compared to those without seizures, indicating that the amount of oxidative stress in patients with fever and seizures was higher than in the control group. The PAB in the case group (febrile children with seizures) had been disturbed compared to the control group (febrile patients without seizures). An increase in oxidative stress and a decrease in the level of antioxidants in patients with fever and seizures, compared to those with fever alone, is a consistent finding in similar studies. However, we used an alternative laboratory method to verify this issue, which is highly accurate and reliable.The results of our study support the hypothesis that if the serum level of antioxidants is low in a febrile child, the probability of fever and seizures in this child is higher than in a similar case with a higher serum antioxidant level. To prove this hypothesis, more extensive studies and larger follow-up are needed.
Ethical Considerations
Compliance with ethical guidelines
The Research Ethics Committee of Sabzevar University of Medical Sciences, Sabzevar, Iran, approved the study protocol (Code: IR.MEDSAB.REC.1398.118). This study adhered to the principles outlined in the Declaration of Helsinki. Informed consent was obtained from the parents or legal guardians of patients.
Funding
This study was supported by the Sabzevar University of Medical Sciences, Sabzevar, Iran (Grant No.: 98036).
Authors' contributions
Conceptualization: Houman Tehrani; Methodology: Mohammad Salari Zare, Mehran Mir, Houman Tehrani, Parastoo Amiri, and Kazem Hassanpour; Writing the original draft: Saeideh Sadat Shobeiri; Investigation, review, editing, and final approval: All authors;
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to the Vice Chancellor of Research and Technology Sabzevar University of Medical Sciences, Sabzevar, Iran.
References
Febrile seizure (FS) is a benignant circumstance that occurs between six and sixty months of age with a temperature of 38 °C or more, which is not a result of central nervous system (CNS) infection or metabolic imbalance and has no history of previous seizures (Bakhtiari et al., 2023). FS is the most common type of seizure in children, with a prevalence of 2–5% (Delpisheh et al., 2014; Rivas-García et al., 2022). Risk factors for FS include premature birth, brain disorders, and family history (Bakhtiari et al., 2023; Sharawat et al., 2016). There are two types of FSs: Simple and complex. A simple FS is an initial generalized seizure, typically tonic-clonic, accompanied by fever, that lasts <15 minutes and does not recur within 24 hours. Complex FSs last at least 15 minutes, are accompanied by focal neurologic symptoms, or reoccur within 24 h (Smith et al., 2019). Various factors contribute to the recurrence of attacks, including age, sex, family and personal history of seizures, body temperature at the time of seizure, and the interval between the onset of fever and seizure (Talebian & Mohammadi, 2009).
Reactive oxygen species (ROS) are a family of unstable molecules composed of oxygen and one or more unpaired electrons in the outermost shell. ROS are highly reactive compounds due to the presence of unpaired electrons (León Navarro et al., 2020). The most prevalent ROS are hydroxyl radicals, superoxide anions, and hydrogen peroxide. In a healthy body, these radicals play a crucial role in cellular communication, development, apoptosis, and systemic functions, such as blood pressure regulation and immunological responses (Brieger et al., 2012; León Navarro et al., 2020). Conversely, oxidative stress occurs when the body produces more ROS than the antioxidant defense system can eliminate. Under these circumstances, basic cell macromolecules, including DNA, lipids, and proteins, can be oxidized (León Navarro et al., 2020). Crucial enzymes may alter both structure and function as a result of protein oxidation (Stadtman, 2001). Lipid peroxidation can change the fluidity, permeability, and protein-membrane functions, leading to hyperexcitability (Wong-Ekkabut et al., 2007). An imbalance between the production of ROS and the antioxidants that scavenge them causes oxidative stress (León Navarro et al., 2020).
Recent research has demonstrated the involvement of lipid peroxidation and free oxygen radicals in the pathophysiology of several diseases. Numerous diseases, including asthma, diabetes mellitus; rheumatologic conditions, such as rheumatoid arthritis and cancer; neurological conditions, including stroke and epilepsy; and inflammatory disorders have all been linked to oxidative stress (Kumar & Kumari, 2017; Leung et al., 2018). The production of lipid peroxidation and free radicals accelerates cell death (Bakhtiari et al., 2023). The body develops defense systems to stop oxidants, such as free radicals and lipid peroxidation, from causing damage. These are the “antioxidant defense systems,” which include glutathione reductase (GR), glutathione peroxidase (GPx), superoxide dismutase (SOD), and catalase (CAT) (Bakhtiari et al., 2023; Fetveit, 2008; Vidailhet et al., 2017) A disturbance in the equilibrium of pro-oxidant antioxidants is commonly referred to oxidative stress, and it plays a role in the development of multiple neurodegenerative diseases, autoimmune disorders, and cancer (Avval et al., 2018). In this regard, the present study aimed to evaluate the pro-oxidant-antioxidant balance (PAB) in febrile children with and without seizures.
2. Materials and Methods
This cross-sectional study was conducted at Heshmatieh Hospital, Sabzevar University of Medical Sciences, Sabzevar, Iran, between March 2020 and March 2021.
Eighty children, aged six months to five years, were selected from among patients admitted to Heshmatieh Hospital in Sabzevar using non-random sampling. Forty febrile children with a temperature of 38 °C and above (F) and 40 febrile children who had experienced their first FS were included. Blood samples were collected from each patient. In the case of patients with fever and seizures, the serum sample was taken in the second hour after the seizure, that is, between one and two hours after the seizure, and in the case of patients with fever and without seizures, the blood sample was taken when the fever was 38 degrees or higher. Patients with seizures without fever and a history of seizures without fever in the past, those suffering from developmental disorders and cerebral palsy, those suffering from metabolic and genetic diseases, and those with syndromes that cause or accompany seizures were excluded. The patient serum samples were prepared and stored at -20 °C until the PAB test was performed.
The PAB test
The PAB test, is a method that simultaneously determines the oxidants and antioxidants of the target sample in a single test (Alamdari et al., 2007). The PAB measurement method in our study involved investigating the activity of both oxidants and antioxidants simultaneously, tetramethylbenzoyl (TMB) was used as an oxidation-reduction index due to its electrochemical and optical properties to evaluate PAB (Boskabadi et al., 2022). The pro-oxidant-antioxidant ratio values were expressed in HK (HK unit, H: Hamidi Alamdari, K: George Koliakos) (Boskabadi et al., 2022). HK is an optional unit that is calculated based on the percentage of hydrogen peroxide absorbed in the standard solution (Samani et al., 2022). An improved PAB was used according to a previously described method (Avval et al., 2018; Boskabadi et al., 2022; Tavana et al., 2016). Briefly, a standard curve was drawn using 0%-100% ratios of 250 μM hydrogen peroxide with 3 μM uric acid (in 10 mM sodium hydroxide). Based on the concentration of hydrogen peroxide in the reaction, the peroxidase enzyme oxidizes the TMB substrate, which is observed as a blue color. At the end of the reaction, hydrochloric acid produced a yellow color at a wavelength of 450 nm. The absorbance was measured at 450 nm with a reference wavelength of 620 nm using an ELISA reader. Finally, pro-oxidant-antioxidant ratio values were expressed in HK units.
Statistical analysis
In the description of the data, appropriate statistical tables and indices, such as Mean±SD, etc. were used. In the analysis of the data, the normality of the data was first investigated using the Shapiro-Wilk test, which confirmed normality. For normal data, appropriate parametric methods, such as student’s t-test, were used. In cases of non-normality, Mann-Whitney and Wilcoxon’s tests were used. The Pearson chi-square test was used for data analysis with nominal scales, and in cases where more than 20% of the expected frequencies in the tables were less than 5 (Cochran), Fisher’s exact test was used. IBM-SPSS software, version 20 was used for the analysis.
3. Results
In this study, 80 patients, including 32 girls (40%) and 48 boys (60%), with a mean age of 36.67±18.12 months and an age range of 6-60 months. HK and fever variables were evaluated in the FS (fever and seizures) and F (fever) groups. The variables of duration of fever, duration of seizures, type of seizures, frequency of seizures, history of seizures, history of epilepsy in first-degree relatives of the patient, history of epilepsy in other relatives of the patient, history of fever and seizures in first-degree relatives of the patient, and history of fever and seizures in other relatives were examined only in the FS group patients.
The age range (maximum and minimum) in both groups was 6 to 60 months. The Mean±SD of age in the FS and F groups was 35.63±18.20 months and 37.73±18.21 months, respectively, and no significant difference was observed between the two groups in terms of age (P=0.567). The number of girls in each of the FS and F groups was 16(40%). The number of boys in each of the FS and F groups was 24(60%). The gender distribution in the studied groups did not differ significantly from one another (P=1.00). Therefore, the two groups were similar in terms of age and sex.
Comparison of HK between FS and F groups
The range of observed HK (the difference between the highest and lowest HK) was 43.54 in the FS group and 66.93 in the F group. The Mean±SD of HK in the FS group was 180.43±9.28, and in the F group was 131.83±17.73. In terms of the average HK, the two groups were significantly different from each other (P<0.001), and the F group had lower HK compared to the FS group (Figure 1).
Comparison of fever between groups
According to the patients’ results, the number of patients with a fever of 38-39 °C was 28(70%) in the FS group and 29(72.5%) in the F group. The number of patients with a fever of >39 °C in the FS and the F groups was 12(30%) and 11(27.5%), respectively. The distribution of patients with varying degrees of fever among the studied groups did not significantly differ from one another (P=0.805).
Comparison of HK between groups of fever degrees according to FS and F groups
In the FS group, the mean HK in the group with a fever of 38-39 °C was lower than the group with a fever over 39 °C, but the difference was not significant (P=0.095). In the F group, the average HK was higher in the group with a fever of 38-39 °C than in the group with a fever >39 °C, but the difference was not significant (P=0.083).
Relationship between age and HK variables
In the FS group, age had an inverse relationship with HK, but the correlation value was not significant (r=-0.032, P=0.845). In the F group, age had a direct relationship with HK; however, the correlation value was not significant (r=0.102, P=0.529).
Comparison of variables between girls and boys in FS group
The frequency distribution of fever and seizures in other relatives of male patients was significantly higher than that in female patients (P=0.027). No significant differences were observed between girls and boys in the frequency distribution of the other variables (Table 1).
Comparison of variables between different groups of fever in FS group
The frequency distribution of the time from the onset of fever to the onset of seizures was significantly different between patients in the group with a temperature of >39 °C and the group with a temperature of 38-39 °C (P=0.013). The frequency distribution of fever and complex seizures was significantly higher in the >39 °C group than in the 38-39 °C (P=0.047). The distribution of the frequency of fever and seizures in 24 h was significantly higher in the 39 °C group than in the 38-39 °C (P<0.001). No significant difference was observed in the frequency distribution of other variables between patients in the group with a temperature of >39 °C and the group with a temperature of 38-39 °C (Table 2).
HK comparison between different variables in FS group
In the FS group, the average HK between the levels of any of the variables of time from the onset of fever to the onset of seizures, duration of seizures, type of fever and seizures, frequency of seizures in the last 24 h, previous history of fever and seizures in the patient, history of epilepsy in first-degree relatives of the patient, history of epilepsy in other relatives of the patient, history of fever and seizures in first-degree relatives, and history of fever and seizures in other relatives of the patient showed no significant difference (P<0.05) (Table 3).
4. Discussion
In this study, 80 patients, including 32 girls (40%) and 48 boys (60%), with a mean age of 36.67±18.12 months and an age range of 6 to 60 months in the groups of febrile patients with and without seizures, were evaluated in terms of HK variables and degree of fever.
In our study, the average age was 36.67±18.12 months, with an age range of 6 to 60 months. Also, the age range (maximum and minimum age) in both groups was 6-60 months. The Mean±SD of age in the FS and F group was 35.63±18.20 months and 37.73±18.21 months, respectively, and no significant difference was observed between the two groups in terms of age. In the study by Iyshwarya et al. (2013), the average age of children with fever and seizures was 3.05±2.19 years; in those with only fever, it was 3.11±1.24 years; and in the control group, it was 3.86±1.18. In the study by Abuhandan et al., the average age was 26.65±12.58 months for the group with fever and seizures and 11.53±30.46 months for the control group. In this study, no statistically significant difference was observed between the two groups in terms of age (Abuhandan et al., 2013). In another study, the average age of patients with fever and seizures was 2.13±0.82 years. In the group of febrile children without seizures, serving as a control, the average age was 2.47±1.16 years, with no significant difference in terms of age (El-Masry et al., 2018).
Our results showed that the number of girls in each of the FS and F groups was 16(40%). The number of boys in each of the FS and F groups was 24(60%). The gender distribution in the studied groups did not differ significantly from one another. In a study by Iyshwarya et al., no significant gender differences were observed in children with fever and seizures (Iyshwarya et al., 2013). In a cross-sectional study conducted in Iran, no significant gender difference was observed regarding FSs in children aged 6 months to 5 years (Ehsanipour et al., 2009). However, Mollah et al. (2008) revealed that male children were more prone to fever and seizures than female children.
In the current study, of 40 patients with fever and seizures (FS group), 34 had simple fever and seizures (85%), and 6 had complex fever and seizures (15%). Similar to our findings, a study by Gϋnes et al. reported that of 31 patients in the fever and seizure group, 25 patients (80%) had simple FSs, and six patients (20%) had complex FSs (Güneş et al., 2009).
FSs are defined as seizures between six and sixty months of age with a temperature of 38 °C or more, which is not a result of CNS infection or metabolic imbalance, and have no history of previous FSs. Many studies have considered factors, such as fever background, seizures in first-degree relatives, micronutrient deficiency, immunological reactions, and oxidative stress as potential aggravating factors (Hartfield, 2010; Pacitti et al., 2013). Seizures are the most common cause of emergency department visits and hospitalizations in children (Salmi et al., 2021). Children with early-onset fever and seizures, especially those with recurrent fever and seizures, may be at greater risk of poorer verbal and processing performance and are therefore at risk of cognitive and functional impairments (Billstedt et al., 2020). A complex interaction among the brain, genetics, epigenetics, and early environment is involved in fever and seizures (Mewasingh et al., 2020). Fever and convulsions are considered responses of the developing brain to fever, but their exact pathophysiology remains unknown. A set of environmental and genetic factors are involved in its creation. Specific mutations in ion channels make individuals susceptible to fever and seizures. Oxidative stress disturbance of the balance between antioxidants and pro-oxidants in the body (Momen Beitollahi et al., 2010). Antioxidants eliminate free radicals in the body. In contrast, compounds that can produce oxygen-free radicals in the body are called pro-oxidants (Kunz, 2002). Some types of free radicals contain nitrogen, while others are produced during harmful processes and contain oxygen, which, upon formation, damages proteins, lipids, and DNA (Momen Beitollahi et al., 2010). In contrast, seizures lead to the production of free radicals. Therefore, oxidative stress and the production of free radicals are currently recognized as key effects of seizures (Valko et al., 2007). Recent data have shown that disorders in the antioxidant system make the nervous system vulnerable and increase a person’s susceptibility to convulsive attacks (Martinc et al., 2012). In other words, free radical production provokes convulsive attacks (Laus et al., 2017).
In this study, pro-oxidant-antioxidant ratio values were expressed in HK units. This optional unit is calculated based on the percentage of hydrogen peroxide absorbed in the standard solution. The Mean±SD of HK in the FS group was 180.43±9.28, and in the F group, it was 131.83±17.73. The two groups were significantly different in terms of the other (P<0.001). Therefore, the amount of HK in patients in the FS group was significantly higher than in patients in the F group, and this proved that the amount of oxidative stress in patients with fever and seizures is higher than in patients with fever but without seizures. The PAB in the FS group was disturbed compared to the F group.
Compared to previous studies, no similar study was found that measured and compared the PAB of serum samples from patients with fever and seizures versus those with fever without seizures using the PAB test. However, in other studies, the levels of antioxidants and the amount of oxidative stress have been measured and compared in patients with fever and seizures, as well as in patients with fever, using other methods. Akarsu et al. measured the levels of erythrocyte arginase, plasma malondialdehyde (MDA), erythrocyte CAT, cerebrospinal fluid MDA, cerebrospinal fluid nitric oxide, and plasma nitric oxide. Their results indicated that the level of free radicals was significantly higher in the FS group than in the control group. Also, the authors showed that the risk of free radicals in seizures without fever was significantly higher than in seizures with fever (Akarsu et al., 2007). In the study by Gϋnes et al., erythrocyte MDA and GPx levels were significantly higher. In contrast, SOD levels were significantly lower, in the group of patients with fever and seizures. This result, consistent with our study’s results, showed a direct relationship between the occurrence of seizures caused by fever and increased levels of free radicals (Güneş et al., 2009). Increased MDA levels indicate the loss of fatty acids, leading to cell membrane damage and cell death. Akarsu et al. investigated the effects of fever and FSs on the oxidant status in children finding that the plasma MDA level was increased in children who had FSs (Akarsu et al., 2007). Moreover, the enzymes SOD and GPx play protective roles against free radicals. Gϋnes et al. showed that SOD levels decreased and GPx levels increased after FSs. Overproduction of superoxide may occur in fever and seizures, and decreased levels of SOD may result in reduced catalysis of superoxide to oxygen and hydrogen peroxide. GPx activity may enhance the conversion of hydrogen peroxide to water as a compensatory mechanism (Güneş et al., 2009). Although it is well-known that seizures cause oxidative stress, the effects of fever and seizures on oxidative balance remain unclear (Akarsu et al., 2007). In Iyshwarya et al.’s study, the increase in the stress marker MDA among children with fever and seizures and the decrease in serum levels of zinc and magnesium as antioxidants in this group, indicated that oxidative stress had increased among those with fever and seizures (Iyshwarya et al., 2013).
In conjunction with our study, Abu-Handan et al. showed that oxidative stress is higher in patients with fever and simple seizures than in healthy individuals, and that it plays a crucial role in the occurrence of FSs (Abuhandan et al., 2013).
5. Conclusion
According to our results, the average serum level of PAB in febrile children with seizures was significantly higher compared to those without seizures, indicating that the amount of oxidative stress in patients with fever and seizures was higher than in the control group. The PAB in the case group (febrile children with seizures) had been disturbed compared to the control group (febrile patients without seizures). An increase in oxidative stress and a decrease in the level of antioxidants in patients with fever and seizures, compared to those with fever alone, is a consistent finding in similar studies. However, we used an alternative laboratory method to verify this issue, which is highly accurate and reliable.The results of our study support the hypothesis that if the serum level of antioxidants is low in a febrile child, the probability of fever and seizures in this child is higher than in a similar case with a higher serum antioxidant level. To prove this hypothesis, more extensive studies and larger follow-up are needed.
Ethical Considerations
Compliance with ethical guidelines
The Research Ethics Committee of Sabzevar University of Medical Sciences, Sabzevar, Iran, approved the study protocol (Code: IR.MEDSAB.REC.1398.118). This study adhered to the principles outlined in the Declaration of Helsinki. Informed consent was obtained from the parents or legal guardians of patients.
Funding
This study was supported by the Sabzevar University of Medical Sciences, Sabzevar, Iran (Grant No.: 98036).
Authors' contributions
Conceptualization: Houman Tehrani; Methodology: Mohammad Salari Zare, Mehran Mir, Houman Tehrani, Parastoo Amiri, and Kazem Hassanpour; Writing the original draft: Saeideh Sadat Shobeiri; Investigation, review, editing, and final approval: All authors;
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors express their gratitude to the Vice Chancellor of Research and Technology Sabzevar University of Medical Sciences, Sabzevar, Iran.
References
Abuhandan, M., Calik, M., Taskin, A., Yetkin, I., Selek, S., & Iscan, A. K. I. N. (2013). The oxidative and antioxidative status of simple febrile seizure patients. JPMA. The Journal of the Pakistan Medical Association, 63(5), 594-597. [PMID]
Akarsu, S., Yilmaz, S., Ozan, S., Kurt, A., Benzer, F., & Gurgoze, M. K. (2007). Effects of febrile and afebrile seizures on oxidant state in children. Pediatric Neurology, 36(5), 307–311. [DOI:10.1016/j.pediatrneurol.2007.01.010] [PMID]
Alamdari, D. H., Paletas, K., Pegiou, T., Sarigianni, M., Befani, C., & Koliakos, G. (2007). A novel assay for the evaluation of the prooxidant-antioxidant balance, before and after antioxidant vitamin administration in type II diabetes patients. Clinical Biochemistry, 40(3-4), 248–254. [DOI:10.1016/j.clinbiochem.2006.10.017] [PMID]
Zahedi Avval, F., Mahmoudi, N., Nosrati Tirkani, A., Jarahi, L., Hamidi Alamdari, D., & Sadjadi, S. A. (2018). Determining pro-oxidant antioxidant balance (PAB) and total antioxidant capacity (TAC) in Patients with schizophrenia. Iranian Journal of Psychiatry, 13(3), 222–226. [PMID]
Bakhtiari, E., Heydarian, F., Azmoudeh, F., Kaffashbashi, M., & Heidarian, M. (2023). Serum level of vitamin A in febrile children with and without seizure: A comparative study. Heliyon, 9(8), e18536. [DOI:10.1016/j.heliyon.2023.e18536] [PMID]
Billstedt, E., Nilsson, G., Leffler, L., Carlsson, L., Olsson, I., & Fernell, E., et al. (2020). Cognitive functioning in a representative cohort of preschool children with febrile seizures. Acta Paediatrica, 109(5), 989–994. [DOI:10.1111/apa.15059] [PMID]
Boskabadi, H., Marefat, M., Maamouri, G., Abrishami, M., Abrishami, M., & Shoeibi, N., et al. (2022). Evaluation of pro-oxidant antioxidant balance in retinopathy of prematurity. Eye, 36(1), 148–152. [DOI:10.1038/s41433-021-01465-6] [PMID]
Brieger, K., Schiavone, S., Miller, F. J., Jr, & Krause, K. H. (2012). Reactive oxygen species: From health to disease. Swiss Medical Weekly, 142, w13659. [DOI:10.4414/smw.2012.13659] [PMID]
Delpisheh, A., Veisani, Y., Sayehmiri, K., & Fayyazi, A. (2014). Febrile seizures: Etiology, prevalence, and geographical variation. Iranian Journal of Child Neurology, 8(3), 30. [PMID]
Ehsanipour, F., Talebi, T. M., Vahid, H. N., & Kani, K. (2009). [Serum zinc level in children with febrile convulsion and its comparison with that of control group (Persian)]. Iranian Journal of Pediatrics, 19(1), 65-68. [Link]
El-Masry, H. M. A., Sadek, A. A., Hassan, M. H., Ameen, H. H., & Ahmed, H. A. (2018). Metabolic profile of oxidative stress and trace elements in febrile seizures among children. Metabolic Brain Disease, 33(5), 1509–1515. [DOI:10.1007/s11011-018-0258-7] [PMID]
Fetveit A. (2008). Assessment of febrile seizures in children. European Journal of Pediatrics, 167(1), 17–27. [DOI:10.1007/s00431-007-0577-x] [PMID]
Güneş, S., Dirik, E., Yiş, U., Seçkin, E., Kuralay, F., & Köse, S., et al. (2009). Oxidant status in children after febrile seizures. Pediatric Neurology, 40(1), 47–49. [DOI:10.1016/j.pediatrneurol.2008.09.006] [PMID]
Hartfield D. (2010). Iron deficiency is a public health problem in Canadian infants and children. Paediatrics & Child Health, 15(6), 347–350. [DOI:10.1093/pch/15.6.347] [PMID]
Iyshwarya, U., Kalyan, P. P., Suma, H., & Aruna, K. R. (2013). Serum trace elements and oxidative stress marker in children with febrile seizure. Journal of Biomedical Sciences, 2(1), 1-5. [Link]
Kumar, I. U., & Kumari, A. (2017). Febrile seizures–can vitamin C act as prophylactic agent?. National Journal of Laboratory Medicine, 6(1), BO01-BO04. [Link]
Kunz W. S. (2002). The role of mitochondria in epileptogenesis. Current Opinion in Neurology, 15(2), 179–184. [DOI:10.1097/00019052-200204000-00009] [PMID]
Laus, M. N., Soccio, M., Alfarano, M., Pasqualone, A., Lenucci, M. S., & Di Miceli, G., et al. (2017). Different effectiveness of two pastas supplemented with either lipophilic or hydrophilic/phenolic antioxidants in affecting serum as evaluated by the novel antioxidant/oxidant balance approach. Food Chemistry, 221, 278–288. [DOI:10.1016/j.foodchem.2016.10.050] [PMID]
León Navarro, D. A., Crespo, M., & Martín, M. (2020). Chapter 6 - Oxidative stress in epileptogenesis: Febrile seizures, chemoconvulsant pilocarpine, and electrical stimulation. In C. R. Martin & V. R. Preedy (Eds.), Oxidative stress and dietary antioxidants in neurological diseases (pp. 81-94). Cambridge: Academic Press. [DOI:10.1016/B978-0-12-817780-8.00006-2]
Leung, A. K., Hon, K. L., & Leung, T. N. (2018). Febrile seizures: An overview. Drugs in Context, 7, 212536. [DOI:10.7573/dic.212536] [PMID]
Martinc, B., Grabnar, I., & Vovk, T. (2012). The role of reactive species in epileptogenesis and influence of antiepileptic drug therapy on oxidative stress. Current Neuropharmacology, 10(4), 328–343. [DOI:10.2174/157015912804499447] [PMID]
Mewasingh, L. D., Chin, R. F. M., & Scott, R. C. (2020). Current understanding of febrile seizures and their long-term outcomes. Developmental Medicine and Child Neurology, 62(11), 1245–1249. [DOI:10.1111/dmcn.14642] [PMID]
Mollah, M. A., Rakshit, S. C., Anwar, K. S., Arslan, M. I., Saha, N., & Ahmed, S., et al. (2008). Zinc concentration in serum and cerebrospinal fluid simultaneously decrease in children with febrile seizure: Findings from a prospective study in Bangladesh. Acta Paediatrica, 97(12), 1707–1711. [DOI:10.1111/j.1651-2227.2008.01001.x] [PMID]
Momen-Beitollahi, J., Mansourian, A., Momen-Heravi, F., Amanlou, M., Obradov, S., & Sahebjamee, M. (2010). Assessment of salivary and serum antioxidant status in patients with recurrent aphthous stomatitis. Medicina Oral, Patologia Oral Y Cirugia Bucal, 15(4), e557–e561. [DOI:10.4317/medoral.15.e557] [PMID]
Pacitti, D., Wang, T., Page, M. M., Martin, S. A., Sweetman, J., & Feldmann, J., et al. (2013). Characterization of cytosolic glutathione peroxidase and phospholipid-hydroperoxide glutathione peroxidase genes in rainbow trout (Oncorhynchus mykiss) and their modulation by in vitro selenium exposure. Aquatic Toxicology, 130-131. [DOI:10.1016/j.aquatox.2012.12.020] [PMID]
Rivas-García, A., Ferrero-García-Loygorri, C., Carrascón González-Pinto, L., Mora-Capín, A. A., Lorente-Romero, J., & Vázquez-López, P. (2022). Simple and complex febrile seizures: Is there such a difference? Management and complications in an emergency department. Neurologia, 37(5), 317–324. [DOI:10.1016/j.nrleng.2019.05.010] [PMID]
Salmi, H., Oulasvirta, J., Rahiala, E., Kuisma, M., Lääperi, M., & Harve, H. (2021). Out-of-hospital seizures in children: A population-based study. Pediatric Emergency Care, 37(12), e1274–e1277. [DOI:10.1097/PEC.0000000000002001] [PMID]
Samani, S. A., Moloudi, M. R., Ramezanzadeh, R., Abdi, M., Nikkhoo, B., & Izadpanah, E., et al. (2022). Oral administration of probiotic enterococcus durans to ameliorate experimental autoimmune encephalomyelitis in mice. Basic and Clinical Neuroscience, 13(1), 35–46. [DOI:10.32598/bcn.2021.1955.1] [PMID]
Sharawat, I. K., Singh, J., Dawman, L., & Singh, A. (2016). Evaluation of risk factors associated with first episode febrile seizure. Journal of Clinical and Diagnostic Research, 10(5), SC10–SC13. [DOI:10.7860/JCDR/2016/18635.7853] [PMID]
Smith, D. K., Sadler, K. P., & Benedum, M. (2019). Febrile seizures: Risks, evaluation, and prognosis. American Family Physician, 99(7), 445-450. [Link]
Stadtman E. R. (2001). Protein oxidation in aging and age-related diseases. Annals of the New York Academy of Sciences, 928, 22–38. [DOI:10.1111/j.1749-6632.2001.tb05632.x] [PMID]
Talebian MD, A., & Mohammadi MD, M. (2009). Febrile seizure: recurrence and risk factors. Iranian Journal of Child Neurology, 1(1), 43-46. [DOI: 10.22037/ijcn.v1i1.1004]
Tavana, S., Amini, S., Hakhamaneshi, M. S., Andalibi, P., Hajir, M. S., & Ardalan, A., et al. (2016). Prooxidant-antioxidant balance in patients with phenylketonuria and its correlation to biochemical and hematological parameters. Journal of Pediatric Endocrinology & Metabolism, 29(6), 675–680. [DOI:10.1515/jpem-2015-0398] [PMID]
Valko, M., Leibfritz, D., Moncol, J., Cronin, M. T., Mazur, M., & Telser, J. (2007). Free radicals and antioxidants in normal physiological functions and human disease. The International Journal of Biochemistry & Cell Biology, 39(1), 44–84. [DOI:10.1016/j.biocel.2006.07.001] [PMID]
Vidailhet, M., Rieu, D., Feillet, F., Bocquet, A., Chouraqui, J. P., & Darmaun, D., et al. (2017). Vitamin A in pediatrics: An update from the nutrition committee of the french society of pediatrics. Archives de Pediatrie, 24(3), 288–297. [DOI:10.1016/j.arcped.2016.11.021] [PMID]
Wong-Ekkabut, J., Xu, Z., Triampo, W., Tang, I. M., Tieleman, D. P., & Monticelli, L. (2007). Effect of lipid peroxidation on the properties of lipid bilayers: A molecular dynamics study. Biophysical Journal, 93(12), 4225–4236. [DOI:10.1529/biophysj.107.112565] [PMID]
Type of Study: Original |
Subject:
Clinical Neuroscience
Received: 2024/05/27 | Accepted: 2024/06/5 | Published: 2025/05/1
Received: 2024/05/27 | Accepted: 2024/06/5 | Published: 2025/05/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
