

Volume 15, Issue 6 (November & December 2024)
BCN 2024, 15(6): 819-832 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Abadi F, Moradi A R, Zarafshan H, Mohamadi M, Sadeghi M. A Comparison of Compensatory and Remediation Cognitive Interventions in Preschoolers With Autism: A Study Protocol for Randomized Controlled Trial. BCN 2024; 15 (6) :819-832
URL: http://bcn.iums.ac.ir/article-1-2615-en.html
URL: http://bcn.iums.ac.ir/article-1-2615-en.html



1- Institute for Cognitive Science Studies (ICSS), Tehran, Iran.
2- Department Clinical Psychology, Faculty of Psychology and Education, Kharazmi University, Tehran, Iran.
3- Psychiatry and Psychology Research Center, Tehran University of Medical Sciences, Tehran, Iran.
2- Department Clinical Psychology, Faculty of Psychology and Education, Kharazmi University, Tehran, Iran.
3- Psychiatry and Psychology Research Center, Tehran University of Medical Sciences, Tehran, Iran.
Keywords: Theory of mind (TOM), Executive function (EF), Remediation cognitive intervention, Compensatory cognitive intervention, Autism
Full-Text [PDF 728 kb]
| Abstract (HTML)

Full-Text:
1. Introduction
Autism spectrum disorder (ASD) is a neurological developmental condition characterized by a deficit in social interactions, verbal and nonverbal communication, and restricted and repetitive patterns of activities and interests (APA, 2013). This research focuses only on autism with high-functioning (HFA). Despite having average and high cognitive abilities, a child with HFA has significant deficits in other domains, such as executive functions (EFs) and theory of mind (TOM) (APA, 2013; Alvares et al., 2020; Devine, et al., 2016). Executive functions refer to higher-order cognitive processes that are critical goal-directed and adaptive behaviors (Carlson, 2005; Zelazo, 2015), which are closely related to social-emotional functions such as TOM (Carlson et al., 2015; Ozonoff & Miller, 1999). TOM is the social-cognitive capacity of humans to attribute mental states to themselves and others to anticipate and interpret behavior (Baron- Cohen et al., 1987; Wellman & Liu, 2004). Longitudinal studies have demonstrated a reciprocal relationship between TOM and core components of EFs, including working memory, inhibitory control, and cognitive flexibility (Carlson et al., 2004; Perner & Lang, 1999). There are some reasons for an association between TOM and EFs. First, both cognitive functions have a common developmental timeline and build-up in preschool. Second, TOM and EFs are covered by a common brain region. Third, autistic individuals have impairments in TOM and EFs (Carlson et al., 2002). Because of the critical role of EFs and TOM in every aspect of human life and academic achievement (Bets et al., 2011), several empirical evidence has been focused on cognitive interventions aimed at enhancing TOM and EFs in preschoolers (Steernman et al., 1996; Wellman et al., 2002; Begeer et al., 2011, 2015; Scionti, et al., 2020). As a result, the development and effectiveness of cognitive training programs for improving TOM and core executive functions may help produce treatment protocols that promote social interactions and quality of life from childhood to adulthood (Beeger et al., 2011; Beeger et al., 2015; de Veld et al., 2017).
Over the last few years, many studies focused on the remarkable effects of cognitive interventions (Rossignoli-Palomeque et al., 2019; Scionti, et al., 2020; Macoun et al., 2021; Pasqalotto et al., 2021). Cognitive interventions most commonly use two approaches to promote and remedy cognitive dysfunction: Process-based and strategy-based approaches. The process-based approach points to remediation cognitive interventions (Kleim & Jones, 2008; Sohlberg et al., 2003), while the strategy-based approach is related to compensatory cognitive interventions (Ylvisaker, 1998; Wykes et al., 2011).
Remediation approaches use a wide range of cognitive tasks and a standard set of exercises to restore impaired cognitive functions. Some remediation programs promote a specific cognitive function (e.g. inhibitory control), while others are extended-based, comprising multiple domains (Kleim & Jones, 2008; Mishra & Gazzaley, 2014). In contrast, compensatory strategies are modifications, and behavioral strategies aim to circumvent cognitive and motivational challenges (Horn & Lewis, 2014; Ylvisaker et al., 2007).
Both approaches have potential and unique benefits; consequently, more recent studies suggest that a combination of compensatory and remediation cognitive intervention can be used in cognitive training programs (Cicerone et al., 2011; Partanen et al., 2015).
According to research evidence, hybrid remediation and compensatory interventions may cause generalized improvements in trained and untrained cognitive functions (i.e. executive skills) than using each of these alone (Macoun et al., 2021; Cicerone et al., 2011; Partanen et al., 2015). As a result, combining process-based and strategy-based approaches can be useful in significant change and the near- and far-transfer (Macoun et al., 2021). Although many studies have focused on cognitive training programs to improve impaired functioning, a closer look at the literature on cognitive interventions reveals several gaps and insufficiencies.
In children with ASD, intervention and rehabilitation programs to improve executive functions are far less than the TOM interventions (Fisher & Happe, 2005; Kenworthy et al., 2014; de Vries et al., 2015). Even though there is a reciprocal correlation between TOM and EFs, no specific hybrid training program for enhancing both EFs and TOM has been developed yet.
A large number of cognitive interventions, especially interventions aimed at improving TOM and EFS, were carried out for school-aged children with ASD (Begger et al., 2011; Hoddenbach et al., 2012; de Veries et al., 2015; de Veld et al., 2017; Caputi et al., 2012; Spaniol et al., 2021). However, cognitive interventions in preschool children with ASD are limited (Fisher & Happe, 2005; Gulsrud et al., 2007; Macoun et al., 2021). Since TOM and EF development milestones are in preschool periods, focusing on improving and promoting impaired cognitive functions (EFs and TOM) during the preschool periods will have a lasting effect on social and cognitive functions at school age (Gibb et al., 2021; Scionti, et al., 2020; Diamond & Lee, 2011).
Most studies have shown that impaired EF and TOM have adverse and substantial outcomes for academic performance, psychosocial adjustment, and everyday behavior. On the other hand, neuropsychological assessments do not provide reliable and comprehensive information about EF and TOM behavioral features in real-world situations. Therefore, to evaluate the effectiveness of cognitive intervention on behaviors in a natural environment, one must use behavioral rating measures of TOM and EF.
In the present trial, the intervention program will address some of the limitations of previous cognitive interventions in children with ASD. A remediation-based intervention will be carried out to improve cognitive functions, such as EFs and TOM. Compensatory-based interventions will be carried out to manage disruptive behaviors, communication, and social interaction. As a result, the present study aims to evaluate EF and TOM via cognitive and behavioral assessments.
Study objectives
This research compares the effects of remediation and compensatory cognitive interventions on EFs and TOM skills in preschool children with autism. We are interested in surveying transfer effects from the cognitive intervention to an untrained domain of TOM and EF (i.e. measures of behavioral outcome).
Primary objectives
To assess the effectiveness of remediation and compensatory cognitive intervention and hybrid remediation and compensatory cognitive intervention on TOM skills.
To assess the effectiveness of remediation and compensatory cognitive intervention and hybrid remediation and compensatory cognitive intervention on EF components (working memory, inhibitory control, cognitive flexibility).
Secondary objectives
To assess the effectiveness of remediation and compensatory cognitive intervention and hybrid remediation and compensatory cognitive intervention on TOM behavioral domains.
To assess the effectiveness of remediation and compensatory cognitive intervention and hybrid remediation and compensatory cognitive intervention on EF behavioral domains.
2. Materials and Methods
Trial design
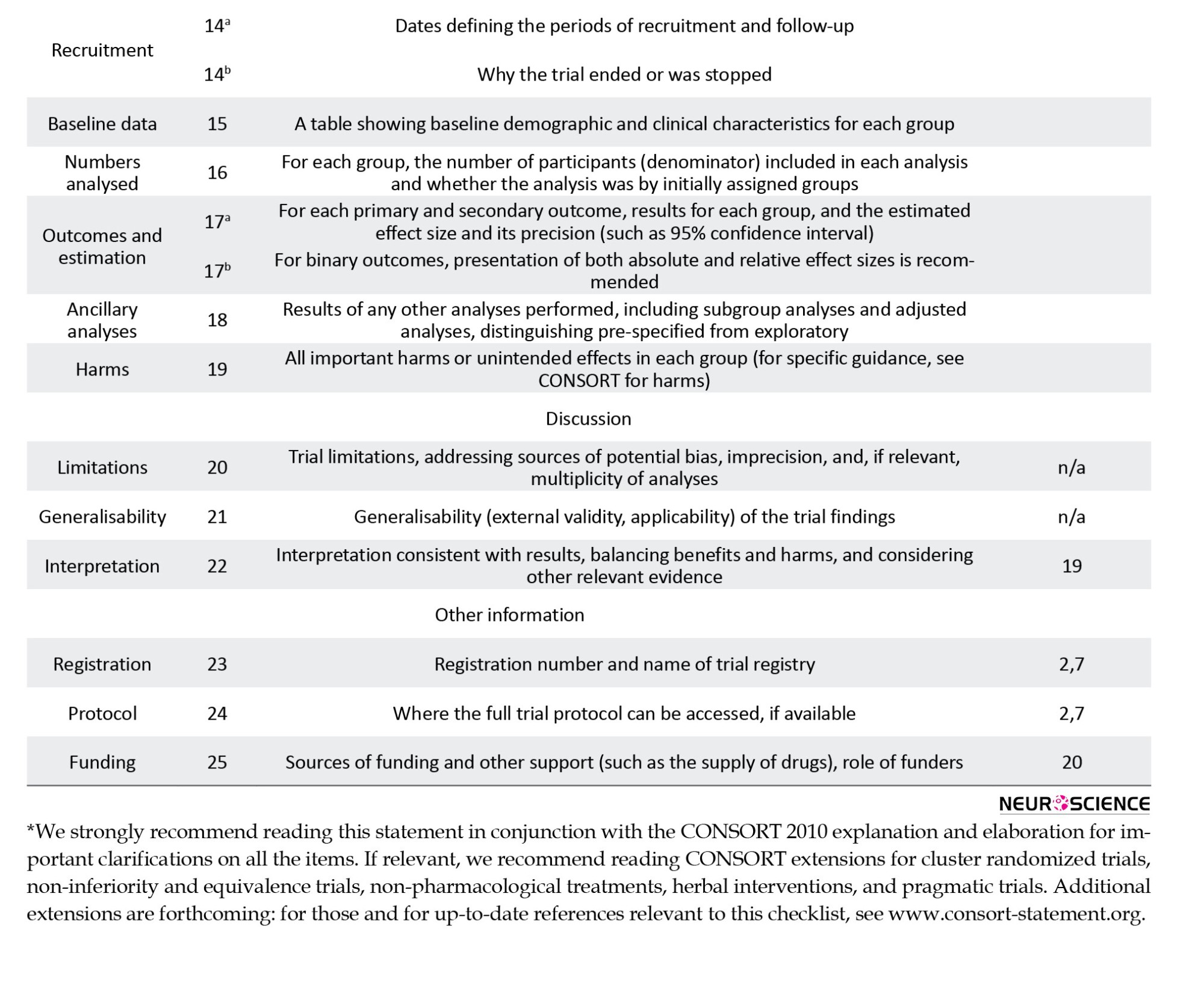
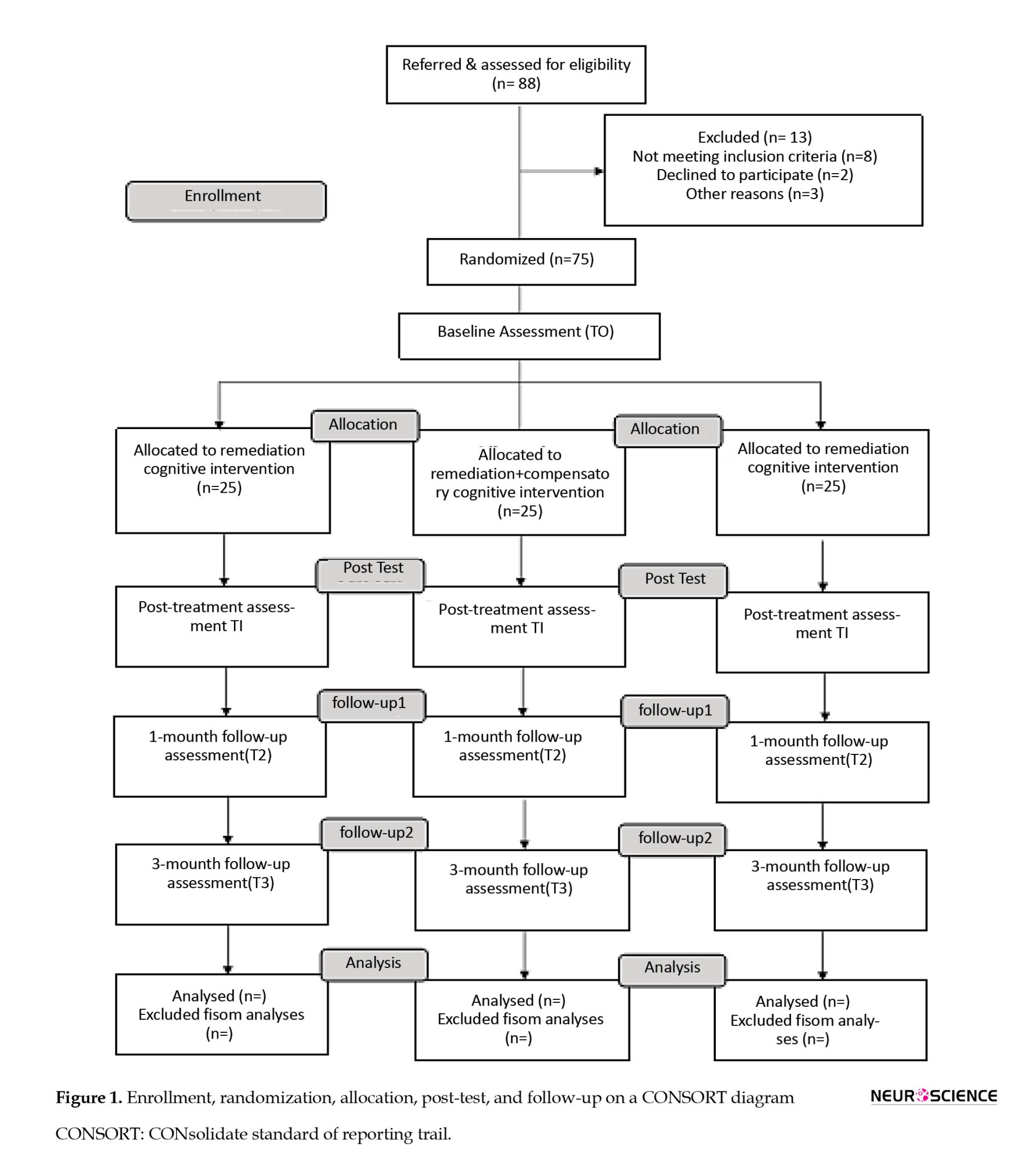
A multicenter, multi-arm, double-blinded, randomized controlled trial will compare the effectiveness of remediation and compensatory cognitive interventions. The proposed trial will have parallel, three groups with random allocation of participants to each group (1:1:1 ratio): Remediation cognitive intervention, compensatory cognitive intervention (active control group), and ‘hybrid’ cognitive intervention (remediation + compensatory). All three arms will be examined at four time points: T0 (pre-test, baseline), T1 (post-test, post-intervention), T2 (1-month follow-up), and T3 (3-month follow-up). The protocol was specified before the start of the trial (Iranian Registry of Clinical Trials [IRCT]) and published before the data collection was finished. Figure 1 outlines this trail’s CONSORT (CONsolidate standard of reporting trail) flow diagram.
Participants and eligibility criteria
Parents of preschoolers with ASD, ages 4 to 7 years, are invited to participate. The diagnostic and statistical manual of mental disorders, fifth edition (DSM-5) is used to diagnose ASD: A multidisciplinary professional team has assessed all children and received a diagnosis of ASD. The inclusion criteria will be as follows: Child aged between 4 and 7 years, a preliminary diagnosis of ASDs (according to psychiatrist criteria from the DSM-5 edition), an intelligence quotient (IQ) of at least 70 as measured by the version of the Persian Wechsler intelligence scale for children (WISC- III), parental consent to participate in research, and availability to participate in the research for six months. The exclusion criteria will be as follows: Participation in a similar rehabilitation and psychological intervention, refusal/withdrawal to participate in this trial, severe sensory motor impairment condition associated with ASD, absence more than three times during the intervention period, no access to the internet at home, and low intrinsic motivation to participate.
Ethics and dissemination
The study protocol was approved by the Human Research Ethics Committee of the Institute of Cognitive Science Studies and Institutional Research. This study was also registered by the Iranian Registry of Clinical Trials (IRCT). All of the participants voluntarily will be joined in the present study and they are asked to fill written informed consent. Participants data will be detected by the code number. Research records will be retained for three years after the completion of the research. Participants will be provided the opportunity to fill out questionnaires and checklists and they are asked to call principal investigator with any question and ambiguity. Training sessions may be recorded on video or photographed and used to educate or present, but the faces of the children will be obscured in both cases. Each participant will be notified of the risk and potential benefits of taking part in this trial.
Recruitment procedure
The principal investigator will be given the details of the study over the phone and via WhatsApp to the parents/caregivers of the children who meet the inclusion criteria. Obviously, individuals may submit an opt-out form if they do not want to be contacted again for research purposes. The principal investigator will contact the participants about two weeks later. The research assistant explains the research details to the parents, such as the sessions’ length and the intervention’s content. Then, they will acquire written permission from the parents to complete questionnaires and checklists during the intervention and follow-up. All intervention and assessment sessions will be conducted using an online Skype meeting app.
Sample size calculation
The sample size for this study will be estimated by power calculations using G*Power software, version 3.1.9.7 (Faul, et al., 2007). Because there are two primary outcomes, the sample size for each primary outcome will be computed separately, and we will use the larger obtained sample size. A previous study indicates that TOM intervention for children with ASD generally has a medium effect size (Cohen’s f=0.260), and previous studies indicate that EF training in preschoolers overall has a medium effect size (Cohen’s d=0.498). The required sample size per arm is 22 (Begeer et al., 2011; Re et al., 2015; Joekar et al., 2017; Volkaert & Noel, 2015). According to our experience in the previous study, a drop-out rate of %15 is assumed so that the sample size will be determined at 25 participants in each group: Remediation group (n=25), remediation + compensatory (n=25), and active control group (n=25).
Randomization and blinding
Sequence generation
After receiving informed consent, all eligible participants will be randomly assigned to one of the three arms using randomized permuted blocks of length 3 in a ratio of 1:1:1. The participants will be randomly allocated and enrolled to arm A, arm B, or arm C. The assignment list will be carried out by a co-principal investigator who is not involved in the present study.
Allocation concealment mechanism
Randomization will be generated by a web-based randomization program. The allocation concealment will be guaranteed, as the arm allocation and randomized sequence list will be provided by the co-principal investigator and will be quite concealed from the research team until the end of the registration period. So, the assignment list will be kept by a responsible person.
Blinding
The research team expects the principal investigator (who is the intervention provider), parents, outcome assessors, and data analyst will be blind to the participant group for the baseline, post-test, as well as a 1-month and 3-month follow-up visit. The research team will not be involved in the randomization process or intervention delivery.
Outcome measures
Primary outcome measures
Inhibitory control and cognitive flexibility assessment
The shape school is intended to evaluate preschoolers’ executive skills, such as cognitive flexibility and inhibitory control. It is planned to orally assess inhibition and switching both independently and concurrently. The shape school is designed in a storybook format with attractive stimuli. The story continues with the pupils “lining up” in the playground, comprised of four conditions. In control conditions, the child is asked to name the figures’ color (i.e. a red circle, a yellow square, or a blue one). In inhibit conditions, shapes have two distinct emotional states. The child is asked to identify pupils who are ready for lunch (happy faces) but not those who are not (sad faces). The inhibit condition evaluates prepotent response suppression. In the switch condition, some pupils wear hats, while others do not. In the third condition, every pupil has a neutral face. The child is asked to identify the shape of the pupils wearing hats and the color of the pupils without hats. The switch condition assesses cognitive shifting. The fourth condition, inhibition, and switching, includes pupils with happy and sad faces and those with and without hats. The child is instructed that not all pupils are prepared to paint. The child is asked to identify the happy pupils who are prepared to paint (e.g. color or shape) but not those with a sad face. In the last condition, response inhibition and cognitive switching are evaluated simultaneously. The efficiency score was calculated (the number of correct- the number of error/total time) (Espy, 1997). The shape school does not have a Persian version. Therefore, their validity and reliability will be calculated.
Working memory assessment
Shape span was used to measure working memory in preschool children. The task was carried out similarly to the digit-span forward and backward, except that line drawing shapes (e.g. animals or fruits) are presented to the child instead of a digit. The digit span was introduced and scored as recommended in the WISC-III manual. In shape span, participants were asked to name a picture of each animal before carrying out the test. If the participant does not identify the animal, the animal is not included in the test. In the beginning, two shapes (one small and one big) are shown to the participant. The participant then is asked to recall the shape from small to large. An image is added at each step to reach 9 images. During the task, the shape of any animal was used only once. The total score is acquired based on the number of correct answers in each trial (Carlson, 2005). The shape span does not have a Persian version. Therefore, their validity and reliability will be calculated.
TOM scale
Wellman and Liu designed the TOM scale to measure some of the TOM’s components. We will use a Persian adaptation of the TOM scale, which consists of six tasks: Diverse desire, diverse belief, knowledge access, explicit false belief, hidden emotion, and content false belief. These five tasks comprise the standard 5-item scale, commonly administered to children aged 3 to 7 years. Each task contains a warm-up or control question in addition to its target question. The translation and adaptation of the TOM scale into the Persian version comprises the following steps: Forward translation, back translation, revision by an expert panel, and pre-testing. The total TOM score is ranging between 0 and 6 (Wellman & Liu, 2004). The TOM scale does not have a Persian version. Therefore, their validity and reliability will be calculated.
TOM story book (TOMSB)
The TOMSB has been chosen to evaluate the TOM quotient of children aged 3 to 11 years. There are 34 tasks with 95 questions, including 77 test questions and 18 justification questions. There are a total of 6 stories: How does Sam feel? Sam goes to the park, Sam goes swimming, Sam visits his grandparents, and Sam on the farm for his birthday celebration. The TOMSBs tasks are based on tasks from previous research, such as emotion recognition, emotion-based desire, mental-physical differentiation, perceptual knowledge, emotion-based belief, and first-order false belief (unexpected transfer and unexpected content task). The translation and adaptation of the TOM quotient into the Persian version comprises the following steps: Forward translation, back translation, revision by an expert panel, and pre-testing. Answers are encoded as correct or incorrect. Internal consistency of the TOM quotient in Dutch samples was good (Cronbach α=0.9) (Blijd-Hoogewys, et al., 2008). The TOM quotient does not have a Persian version. Therefore, its validity and reliability will be calculated.
Secondary outcome measures
TOM behavior checklist (TOMBC)
TOMBC is chosen to evaluate TOM behaviors. The TOMBC is a parent questionnaire meant to examine parental observations of their child’s TOM-related behaviors. Parents are asked to rate the frequency of eight behavioral domains (empathizing with others, inquiring about others’ feelings, apologizing for mistakes, paying attention to what others are saying, unconsciously complimenting others, expressing interest and enthusiasm in what others are saying, asking interesting questions, and understanding jokes) over the previous week (0=never to 5=always). These behaviors were chosen based on information supplied by parents during earlier intervention evaluation sessions. The internal reliability of the TOMBC in Dutch samples was 0.81 (Begeer et al., 2011). The TOM behavior checklist does not have a Persian version. Therefore, its validity and reliability will be calculated.
BRIEF-preschool version
The behavior rating inventory of executive function (BRIEF) questionnaire assesses the different aspects of executive functions in preschool children 2 to 5 years and 11 months in everyday life situations. The preschool version of the behavior assessment test in EF has 63 questions. EFs in this questionnaire are divided into 9 items. Its five clinical scales are inhibit, shift, emotional control, working memory, and planning/organizing. Its three principal clinical signs result from a complex interaction of critical components such as inhibitory self-control, flexibility, and emergent metacognition. Internal consistency and content validity of the BRIEF in Persian samples were good (Cronbach α: 0.93) (Gioia, et al., 2000).
Other measures, diagnostic assessments
Autism treatment evaluation checklist evaluation structure
The autism treatment evaluation checklist (ATEC) is a questionnaire given by parents, teachers, and caregivers to assess changes in the severity of ASD in response to treatment. This questionnaire comprises the overall score (77) as well as the four subscale scores, which are speech/language communication (14 questions), sociability (20 items), sensory/cognitive awareness (18 items), and health/physical/behavioral awareness (18 things) (25 items). A lower score indicates less severe ASD symptoms, and a higher score is associated with more severe ASD symptoms. ATEC is a practical tool to evaluate the effectiveness of various autism treatments. In addition, it is a diagnostic tool for evaluating children’s autism symptoms. Many parents and teachers use ATEC to monitor their child’s performance. Internal consistency and content validity of the ATEC in Persian samples were good (Cronbach α: 0.86 -0.93; Memari et al., 2013).
Wechsler preschool and primary scale
For preschool-aged children, the Wechsler preschool and Primary Scale of Intelligence (WPPSI-III) is an international multidimensional measure of intelligence (from 2 years and 6 months to 7 years and 3 months). The Iranian children will be assessed using the revised Persian Wechsler intelligence scale (Wechsler & Kort 2005). The reliability values for the Persian version are 0.83, 0.90, and 0.88 for verbal IQ, performance IQ, and full-scale IQ (Shahim, 2006).
Intervention description
Remediation cognitive intervention
Autism Yar is a paper and pencil cognitive rehabilitation program (Abadi, et al., 2022). The Autism Yar program introduces a set of tasks and activities that develop and enhance EFs and social cognition skills enjoyably and interactively. EF and memory pack comprise the following workbooks: Working memory, inhibitory control, cognitive flexibility, visual memory, visual-spatial memory, visual-sequential memory, auditory memory, and auditory comprehension. The social cognition pack includes the following workbooks: Emotion comprehension (emotion recognition, situation-based emotion, external cause of the emotion, desire-based emotion, belief-based emotion, reminder of emotion, emotion regulation, hidden emotion, mixed emotion, multiple emotion, emotion caused by moral and immoral factors), appearance-reality distinction, mental physical distinction, diverse desire and diverse belief, informational state (simple visual perspective taking, complex visual perspective taking, seeing leads to knowing, action based knowledge, false belief), and empathy.
The Autism Yar program is a 42-session individual or group-based intervention for children with autism. Due to the COVID-19 pandemic, the intervention will be carried out online by one of the researchers, who will provide training to intervention groups. The online format as a group will be held during 45 sessions (3 days a week) for parents of autistic children. In each online group, there will be about 25 people (Table 1).
Ten sessions (3,6,9,18,21,24,27,30,33,36,39, 42) out of the total sessions will be dedicated to answering parents’ questions. Also, the therapist will do the exercises in the presence of the parents, with one of the children chosen as a model so that they can be trained.
Compensatory cognitive intervention
Compensatory cognitive intervention is based on parent education programs (PEP) and Project ImPACT (improving parents as communication teachers). PEP and Project ImPACT focus on the core symptom areas of ASD (such as behavioral difficulties, socialization, and communication). This program will be conducted and managed by a psychologist (a research team member) consisting of 12 (60-90 minutes) core sessions. The structured PEP sessions can be administered either individually or in groups to the parent using direct strategies, role play, filling out the daily activity schedule, video examples, and homework assignments. Parents are instructed on the underlying causes of autism disorder, the behavioral problems, how to improve the child’s impaired social and cognitive functions, and also behavior management skills. Ingersoll and Dvortcsak detail the intervention strategies and training programs for parents (Ingersoll & Wainer, 2013). Furthermore, during the sessions, the parents will be taught about using positive behavior support techniques to manage maladaptive behaviors and support the improvement of their child’s communication skills, play skills, and social functioning (Table 2) (Brereton & Tonge, 2005).
Hybrid cognitive intervention (compensatory cognitive intervention and remediation cognitive intervention)
This group of children will receive a combination of the Autism Yar program, parent education programs (PEP), and Project ImPACT over 14 weeks (4 days a week). Participants will receive the Autism Yar program 3 days a week, and the PEP will be received one day per week.
Data analysis
Before analysis, the normality of the raw data will be tested for all key variables. The primary and secondary outcomes will be analyzed using repeated measures analysis of variance (ANOVA) and mixed models as the primary design. Multiple imputations will be used for missing observations at post-test, 1-month, and 3-month follow-up. Pre-test differences in demographic characteristics (age, gender, total IQ, verbal IQ, performance IQ, parental education, and parental age) will be investigated with the chi-square tests and ANOVA. Both within (changes within-person across time) and between-subject (changes between persons in the intervention condition versus the control conditions) impacts will be investigated to determine the efficacy of the remediation and compensatory cognitive intervention. The within-subject variable “time” has four levels: T0 (pre-test), T1 (post-test), T2 (1-month follow-up), and T3 (3-month follow-up). The between-subject variable “condition” has two levels: Intervention conditions and control conditions. The eta square statistic (ŋ2) will be computed to estimate the effect size and recognize the practical significance of the results. Secondary outcomes are investigated similarly to the primary outcomes analysis. Statistical analyses were performed using SPSS software, version 22, and the two-sided P was set at 0.05.
3. Discussion
This trial aims to determine the effectiveness of an Autism Yar rehabilitation program for improving EFs and TOM skills in preschoolers with ASD. The Autism Yar can also be used as an educational and rehabilitation tool for teachers and parents by providing them with strategies to create regular and continuous learning opportunities for their children daily at home and school. Overall, the Autism Yar can intensify the positive impact of any developmental, social, and behavioral program for the treatment of ASD children (Fisher & Happe, 2005; Beeger et al., 2015).
The results of this trial will provide evidence to assess the feasibility of parents becoming therapists for their children with ASD through a rigorous yet pragmatic evaluation process. It will also provide evidence for the effectiveness of the Autism Yar program in improving trajectories for children with autism at school age (Beeger et al., 2015).
The strengths of our current trial include its multicenter, randomization, double-blinded, treatment-as-usual to control group, parallel-group trial for the comprehensive evaluation and effectiveness of a dimensional rehabilitation program in preschoolers with autism. Another strength is using multiple outcome assessment tools to obtain information from various reporters.
Three potential limitations of the present trial should be mentioned. First, trained parents will do the intervention. To confirm the rehabilitation program’s effectiveness and generalizability, the training teachers implemented should be evaluated. Second, it will not address whether the rehabilitation group’s TOM and EF gains were sustained or whether the rehabilitation program was associated with greater academic achievement and school readiness at the end of kindergarten and grade 1. It is necessary to focus future studies on the effectiveness of TOM and EFs training on academic achievement and social communication.
Third, although having an active control group is better than an inactive control group, the number of intervention sessions in the active control group (12 sessions) is not the same as the intervention groups (one received 42 sessions and the other received 54 sessions). Therefore, the improvement in performance and changes in brain activity in the intervention groups are probably partially explained by the difference in the amount of intervention between the three groups. So, the groups should receive the same intervention sessions in future studies.
Ethical Considerations
Compliance with ethical guidelines
The study protocol was approved by the Human Research Ethics Committee of the Institute of Cognitive Science Studies and Institutional Research Ethics Committee (Code: IR.UT.IRICSS.REC.1399.011). This study was also registered by the Iranian Registry of Clinical Trials (IRCT) (Code: 20210619051618N1).
Funding
This study has received funding from the Cognitive Science and Technologies Council for conducting parenting workshops, designing the trial, collecting, analyzing, and interpreting data, and developing and designing the Autism Yar rehabilitation program (Project Grant No.: 9598).
Authors' contributions
Conceptualization: Fateme Abadi, Alireza Moradi and Hadi Zarafshan; The trial design: All Authors; Methodolgy: Fateme Abadi, Meysam Sadeghi, Hadi Zarafshan and Mohamadreza Mohammadi; Data collection: Fateme abadi; Data analysis: Fateme Abadi and Meysam Sadeghi; Writing the original draft: Fateme Abadi, Alireza Moradi and Hadi Zarafshan; Review and editing: Fateme abadi and Alireza Moradi; Funding administration: Fateme Abadi and Alireza Moradi; Supervision: Alireza Moradi and Hadi Zarafshan.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the rehabilitation centers for referring their patients to the principal researcher in this study.
References
Autism spectrum disorder (ASD) is a neurological developmental condition characterized by a deficit in social interactions, verbal and nonverbal communication, and restricted and repetitive patterns of activities and interests (APA, 2013). This research focuses only on autism with high-functioning (HFA). Despite having average and high cognitive abilities, a child with HFA has significant deficits in other domains, such as executive functions (EFs) and theory of mind (TOM) (APA, 2013; Alvares et al., 2020; Devine, et al., 2016). Executive functions refer to higher-order cognitive processes that are critical goal-directed and adaptive behaviors (Carlson, 2005; Zelazo, 2015), which are closely related to social-emotional functions such as TOM (Carlson et al., 2015; Ozonoff & Miller, 1999). TOM is the social-cognitive capacity of humans to attribute mental states to themselves and others to anticipate and interpret behavior (Baron- Cohen et al., 1987; Wellman & Liu, 2004). Longitudinal studies have demonstrated a reciprocal relationship between TOM and core components of EFs, including working memory, inhibitory control, and cognitive flexibility (Carlson et al., 2004; Perner & Lang, 1999). There are some reasons for an association between TOM and EFs. First, both cognitive functions have a common developmental timeline and build-up in preschool. Second, TOM and EFs are covered by a common brain region. Third, autistic individuals have impairments in TOM and EFs (Carlson et al., 2002). Because of the critical role of EFs and TOM in every aspect of human life and academic achievement (Bets et al., 2011), several empirical evidence has been focused on cognitive interventions aimed at enhancing TOM and EFs in preschoolers (Steernman et al., 1996; Wellman et al., 2002; Begeer et al., 2011, 2015; Scionti, et al., 2020). As a result, the development and effectiveness of cognitive training programs for improving TOM and core executive functions may help produce treatment protocols that promote social interactions and quality of life from childhood to adulthood (Beeger et al., 2011; Beeger et al., 2015; de Veld et al., 2017).
Over the last few years, many studies focused on the remarkable effects of cognitive interventions (Rossignoli-Palomeque et al., 2019; Scionti, et al., 2020; Macoun et al., 2021; Pasqalotto et al., 2021). Cognitive interventions most commonly use two approaches to promote and remedy cognitive dysfunction: Process-based and strategy-based approaches. The process-based approach points to remediation cognitive interventions (Kleim & Jones, 2008; Sohlberg et al., 2003), while the strategy-based approach is related to compensatory cognitive interventions (Ylvisaker, 1998; Wykes et al., 2011).
Remediation approaches use a wide range of cognitive tasks and a standard set of exercises to restore impaired cognitive functions. Some remediation programs promote a specific cognitive function (e.g. inhibitory control), while others are extended-based, comprising multiple domains (Kleim & Jones, 2008; Mishra & Gazzaley, 2014). In contrast, compensatory strategies are modifications, and behavioral strategies aim to circumvent cognitive and motivational challenges (Horn & Lewis, 2014; Ylvisaker et al., 2007).
Both approaches have potential and unique benefits; consequently, more recent studies suggest that a combination of compensatory and remediation cognitive intervention can be used in cognitive training programs (Cicerone et al., 2011; Partanen et al., 2015).
According to research evidence, hybrid remediation and compensatory interventions may cause generalized improvements in trained and untrained cognitive functions (i.e. executive skills) than using each of these alone (Macoun et al., 2021; Cicerone et al., 2011; Partanen et al., 2015). As a result, combining process-based and strategy-based approaches can be useful in significant change and the near- and far-transfer (Macoun et al., 2021). Although many studies have focused on cognitive training programs to improve impaired functioning, a closer look at the literature on cognitive interventions reveals several gaps and insufficiencies.
In children with ASD, intervention and rehabilitation programs to improve executive functions are far less than the TOM interventions (Fisher & Happe, 2005; Kenworthy et al., 2014; de Vries et al., 2015). Even though there is a reciprocal correlation between TOM and EFs, no specific hybrid training program for enhancing both EFs and TOM has been developed yet.
A large number of cognitive interventions, especially interventions aimed at improving TOM and EFS, were carried out for school-aged children with ASD (Begger et al., 2011; Hoddenbach et al., 2012; de Veries et al., 2015; de Veld et al., 2017; Caputi et al., 2012; Spaniol et al., 2021). However, cognitive interventions in preschool children with ASD are limited (Fisher & Happe, 2005; Gulsrud et al., 2007; Macoun et al., 2021). Since TOM and EF development milestones are in preschool periods, focusing on improving and promoting impaired cognitive functions (EFs and TOM) during the preschool periods will have a lasting effect on social and cognitive functions at school age (Gibb et al., 2021; Scionti, et al., 2020; Diamond & Lee, 2011).
Most studies have shown that impaired EF and TOM have adverse and substantial outcomes for academic performance, psychosocial adjustment, and everyday behavior. On the other hand, neuropsychological assessments do not provide reliable and comprehensive information about EF and TOM behavioral features in real-world situations. Therefore, to evaluate the effectiveness of cognitive intervention on behaviors in a natural environment, one must use behavioral rating measures of TOM and EF.
In the present trial, the intervention program will address some of the limitations of previous cognitive interventions in children with ASD. A remediation-based intervention will be carried out to improve cognitive functions, such as EFs and TOM. Compensatory-based interventions will be carried out to manage disruptive behaviors, communication, and social interaction. As a result, the present study aims to evaluate EF and TOM via cognitive and behavioral assessments.
Study objectives
This research compares the effects of remediation and compensatory cognitive interventions on EFs and TOM skills in preschool children with autism. We are interested in surveying transfer effects from the cognitive intervention to an untrained domain of TOM and EF (i.e. measures of behavioral outcome).
Primary objectives
To assess the effectiveness of remediation and compensatory cognitive intervention and hybrid remediation and compensatory cognitive intervention on TOM skills.
To assess the effectiveness of remediation and compensatory cognitive intervention and hybrid remediation and compensatory cognitive intervention on EF components (working memory, inhibitory control, cognitive flexibility).
Secondary objectives
To assess the effectiveness of remediation and compensatory cognitive intervention and hybrid remediation and compensatory cognitive intervention on TOM behavioral domains.
To assess the effectiveness of remediation and compensatory cognitive intervention and hybrid remediation and compensatory cognitive intervention on EF behavioral domains.
2. Materials and Methods
Trial design
A multicenter, multi-arm, double-blinded, randomized controlled trial will compare the effectiveness of remediation and compensatory cognitive interventions. The proposed trial will have parallel, three groups with random allocation of participants to each group (1:1:1 ratio): Remediation cognitive intervention, compensatory cognitive intervention (active control group), and ‘hybrid’ cognitive intervention (remediation + compensatory). All three arms will be examined at four time points: T0 (pre-test, baseline), T1 (post-test, post-intervention), T2 (1-month follow-up), and T3 (3-month follow-up). The protocol was specified before the start of the trial (Iranian Registry of Clinical Trials [IRCT]) and published before the data collection was finished. Figure 1 outlines this trail’s CONSORT (CONsolidate standard of reporting trail) flow diagram.
Participants and eligibility criteria
Parents of preschoolers with ASD, ages 4 to 7 years, are invited to participate. The diagnostic and statistical manual of mental disorders, fifth edition (DSM-5) is used to diagnose ASD: A multidisciplinary professional team has assessed all children and received a diagnosis of ASD. The inclusion criteria will be as follows: Child aged between 4 and 7 years, a preliminary diagnosis of ASDs (according to psychiatrist criteria from the DSM-5 edition), an intelligence quotient (IQ) of at least 70 as measured by the version of the Persian Wechsler intelligence scale for children (WISC- III), parental consent to participate in research, and availability to participate in the research for six months. The exclusion criteria will be as follows: Participation in a similar rehabilitation and psychological intervention, refusal/withdrawal to participate in this trial, severe sensory motor impairment condition associated with ASD, absence more than three times during the intervention period, no access to the internet at home, and low intrinsic motivation to participate.
Ethics and dissemination
The study protocol was approved by the Human Research Ethics Committee of the Institute of Cognitive Science Studies and Institutional Research. This study was also registered by the Iranian Registry of Clinical Trials (IRCT). All of the participants voluntarily will be joined in the present study and they are asked to fill written informed consent. Participants data will be detected by the code number. Research records will be retained for three years after the completion of the research. Participants will be provided the opportunity to fill out questionnaires and checklists and they are asked to call principal investigator with any question and ambiguity. Training sessions may be recorded on video or photographed and used to educate or present, but the faces of the children will be obscured in both cases. Each participant will be notified of the risk and potential benefits of taking part in this trial.
Recruitment procedure
The principal investigator will be given the details of the study over the phone and via WhatsApp to the parents/caregivers of the children who meet the inclusion criteria. Obviously, individuals may submit an opt-out form if they do not want to be contacted again for research purposes. The principal investigator will contact the participants about two weeks later. The research assistant explains the research details to the parents, such as the sessions’ length and the intervention’s content. Then, they will acquire written permission from the parents to complete questionnaires and checklists during the intervention and follow-up. All intervention and assessment sessions will be conducted using an online Skype meeting app.
Sample size calculation
The sample size for this study will be estimated by power calculations using G*Power software, version 3.1.9.7 (Faul, et al., 2007). Because there are two primary outcomes, the sample size for each primary outcome will be computed separately, and we will use the larger obtained sample size. A previous study indicates that TOM intervention for children with ASD generally has a medium effect size (Cohen’s f=0.260), and previous studies indicate that EF training in preschoolers overall has a medium effect size (Cohen’s d=0.498). The required sample size per arm is 22 (Begeer et al., 2011; Re et al., 2015; Joekar et al., 2017; Volkaert & Noel, 2015). According to our experience in the previous study, a drop-out rate of %15 is assumed so that the sample size will be determined at 25 participants in each group: Remediation group (n=25), remediation + compensatory (n=25), and active control group (n=25).
Randomization and blinding
Sequence generation
After receiving informed consent, all eligible participants will be randomly assigned to one of the three arms using randomized permuted blocks of length 3 in a ratio of 1:1:1. The participants will be randomly allocated and enrolled to arm A, arm B, or arm C. The assignment list will be carried out by a co-principal investigator who is not involved in the present study.
Allocation concealment mechanism
Randomization will be generated by a web-based randomization program. The allocation concealment will be guaranteed, as the arm allocation and randomized sequence list will be provided by the co-principal investigator and will be quite concealed from the research team until the end of the registration period. So, the assignment list will be kept by a responsible person.
Blinding
The research team expects the principal investigator (who is the intervention provider), parents, outcome assessors, and data analyst will be blind to the participant group for the baseline, post-test, as well as a 1-month and 3-month follow-up visit. The research team will not be involved in the randomization process or intervention delivery.
Outcome measures
Primary outcome measures
Inhibitory control and cognitive flexibility assessment
The shape school is intended to evaluate preschoolers’ executive skills, such as cognitive flexibility and inhibitory control. It is planned to orally assess inhibition and switching both independently and concurrently. The shape school is designed in a storybook format with attractive stimuli. The story continues with the pupils “lining up” in the playground, comprised of four conditions. In control conditions, the child is asked to name the figures’ color (i.e. a red circle, a yellow square, or a blue one). In inhibit conditions, shapes have two distinct emotional states. The child is asked to identify pupils who are ready for lunch (happy faces) but not those who are not (sad faces). The inhibit condition evaluates prepotent response suppression. In the switch condition, some pupils wear hats, while others do not. In the third condition, every pupil has a neutral face. The child is asked to identify the shape of the pupils wearing hats and the color of the pupils without hats. The switch condition assesses cognitive shifting. The fourth condition, inhibition, and switching, includes pupils with happy and sad faces and those with and without hats. The child is instructed that not all pupils are prepared to paint. The child is asked to identify the happy pupils who are prepared to paint (e.g. color or shape) but not those with a sad face. In the last condition, response inhibition and cognitive switching are evaluated simultaneously. The efficiency score was calculated (the number of correct- the number of error/total time) (Espy, 1997). The shape school does not have a Persian version. Therefore, their validity and reliability will be calculated.
Working memory assessment
Shape span was used to measure working memory in preschool children. The task was carried out similarly to the digit-span forward and backward, except that line drawing shapes (e.g. animals or fruits) are presented to the child instead of a digit. The digit span was introduced and scored as recommended in the WISC-III manual. In shape span, participants were asked to name a picture of each animal before carrying out the test. If the participant does not identify the animal, the animal is not included in the test. In the beginning, two shapes (one small and one big) are shown to the participant. The participant then is asked to recall the shape from small to large. An image is added at each step to reach 9 images. During the task, the shape of any animal was used only once. The total score is acquired based on the number of correct answers in each trial (Carlson, 2005). The shape span does not have a Persian version. Therefore, their validity and reliability will be calculated.
TOM scale
Wellman and Liu designed the TOM scale to measure some of the TOM’s components. We will use a Persian adaptation of the TOM scale, which consists of six tasks: Diverse desire, diverse belief, knowledge access, explicit false belief, hidden emotion, and content false belief. These five tasks comprise the standard 5-item scale, commonly administered to children aged 3 to 7 years. Each task contains a warm-up or control question in addition to its target question. The translation and adaptation of the TOM scale into the Persian version comprises the following steps: Forward translation, back translation, revision by an expert panel, and pre-testing. The total TOM score is ranging between 0 and 6 (Wellman & Liu, 2004). The TOM scale does not have a Persian version. Therefore, their validity and reliability will be calculated.
TOM story book (TOMSB)
The TOMSB has been chosen to evaluate the TOM quotient of children aged 3 to 11 years. There are 34 tasks with 95 questions, including 77 test questions and 18 justification questions. There are a total of 6 stories: How does Sam feel? Sam goes to the park, Sam goes swimming, Sam visits his grandparents, and Sam on the farm for his birthday celebration. The TOMSBs tasks are based on tasks from previous research, such as emotion recognition, emotion-based desire, mental-physical differentiation, perceptual knowledge, emotion-based belief, and first-order false belief (unexpected transfer and unexpected content task). The translation and adaptation of the TOM quotient into the Persian version comprises the following steps: Forward translation, back translation, revision by an expert panel, and pre-testing. Answers are encoded as correct or incorrect. Internal consistency of the TOM quotient in Dutch samples was good (Cronbach α=0.9) (Blijd-Hoogewys, et al., 2008). The TOM quotient does not have a Persian version. Therefore, its validity and reliability will be calculated.
Secondary outcome measures
TOM behavior checklist (TOMBC)
TOMBC is chosen to evaluate TOM behaviors. The TOMBC is a parent questionnaire meant to examine parental observations of their child’s TOM-related behaviors. Parents are asked to rate the frequency of eight behavioral domains (empathizing with others, inquiring about others’ feelings, apologizing for mistakes, paying attention to what others are saying, unconsciously complimenting others, expressing interest and enthusiasm in what others are saying, asking interesting questions, and understanding jokes) over the previous week (0=never to 5=always). These behaviors were chosen based on information supplied by parents during earlier intervention evaluation sessions. The internal reliability of the TOMBC in Dutch samples was 0.81 (Begeer et al., 2011). The TOM behavior checklist does not have a Persian version. Therefore, its validity and reliability will be calculated.
BRIEF-preschool version
The behavior rating inventory of executive function (BRIEF) questionnaire assesses the different aspects of executive functions in preschool children 2 to 5 years and 11 months in everyday life situations. The preschool version of the behavior assessment test in EF has 63 questions. EFs in this questionnaire are divided into 9 items. Its five clinical scales are inhibit, shift, emotional control, working memory, and planning/organizing. Its three principal clinical signs result from a complex interaction of critical components such as inhibitory self-control, flexibility, and emergent metacognition. Internal consistency and content validity of the BRIEF in Persian samples were good (Cronbach α: 0.93) (Gioia, et al., 2000).
Other measures, diagnostic assessments
Autism treatment evaluation checklist evaluation structure
The autism treatment evaluation checklist (ATEC) is a questionnaire given by parents, teachers, and caregivers to assess changes in the severity of ASD in response to treatment. This questionnaire comprises the overall score (77) as well as the four subscale scores, which are speech/language communication (14 questions), sociability (20 items), sensory/cognitive awareness (18 items), and health/physical/behavioral awareness (18 things) (25 items). A lower score indicates less severe ASD symptoms, and a higher score is associated with more severe ASD symptoms. ATEC is a practical tool to evaluate the effectiveness of various autism treatments. In addition, it is a diagnostic tool for evaluating children’s autism symptoms. Many parents and teachers use ATEC to monitor their child’s performance. Internal consistency and content validity of the ATEC in Persian samples were good (Cronbach α: 0.86 -0.93; Memari et al., 2013).
Wechsler preschool and primary scale
For preschool-aged children, the Wechsler preschool and Primary Scale of Intelligence (WPPSI-III) is an international multidimensional measure of intelligence (from 2 years and 6 months to 7 years and 3 months). The Iranian children will be assessed using the revised Persian Wechsler intelligence scale (Wechsler & Kort 2005). The reliability values for the Persian version are 0.83, 0.90, and 0.88 for verbal IQ, performance IQ, and full-scale IQ (Shahim, 2006).
Intervention description
Remediation cognitive intervention
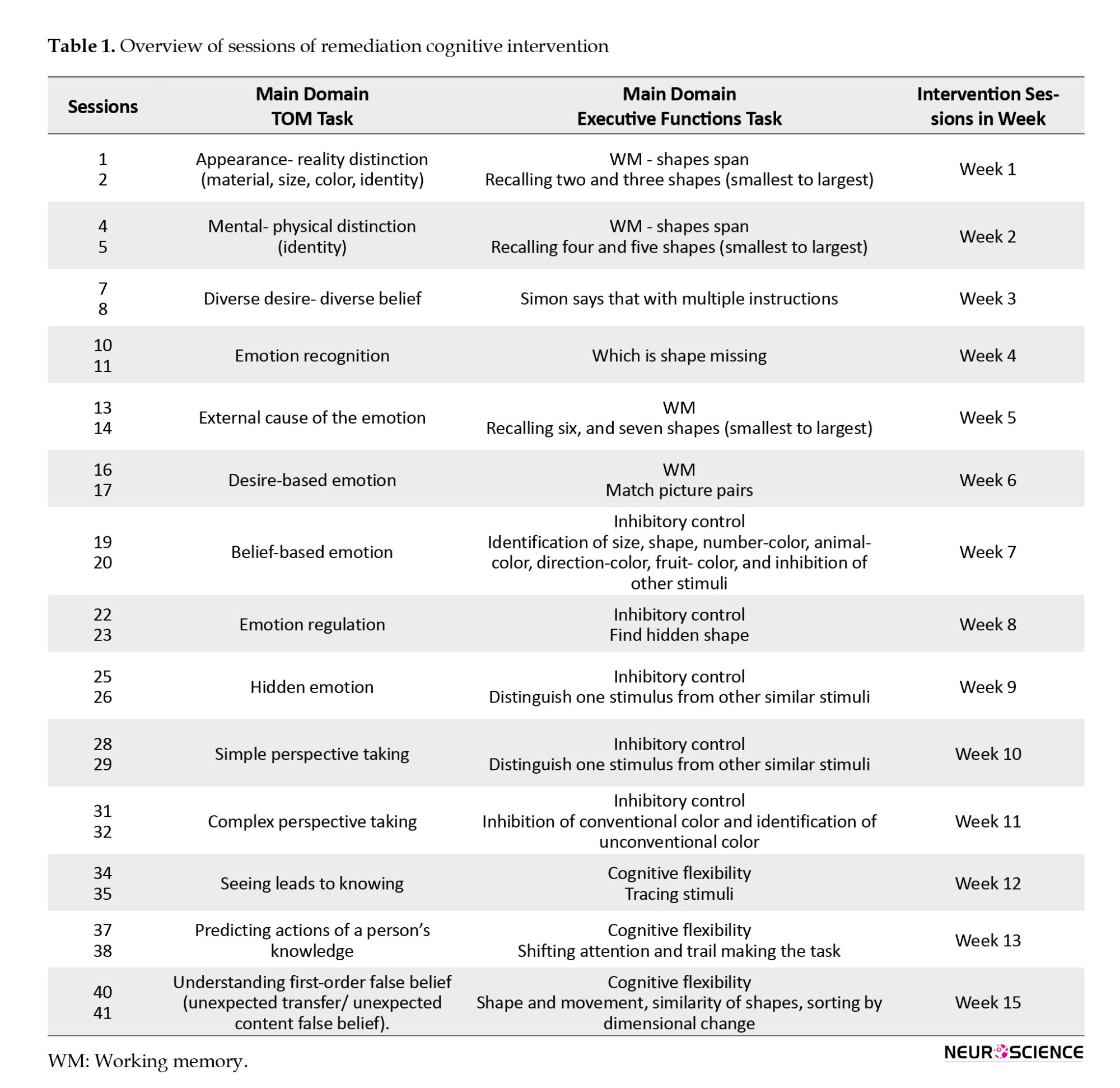
Autism Yar is a paper and pencil cognitive rehabilitation program (Abadi, et al., 2022). The Autism Yar program introduces a set of tasks and activities that develop and enhance EFs and social cognition skills enjoyably and interactively. EF and memory pack comprise the following workbooks: Working memory, inhibitory control, cognitive flexibility, visual memory, visual-spatial memory, visual-sequential memory, auditory memory, and auditory comprehension. The social cognition pack includes the following workbooks: Emotion comprehension (emotion recognition, situation-based emotion, external cause of the emotion, desire-based emotion, belief-based emotion, reminder of emotion, emotion regulation, hidden emotion, mixed emotion, multiple emotion, emotion caused by moral and immoral factors), appearance-reality distinction, mental physical distinction, diverse desire and diverse belief, informational state (simple visual perspective taking, complex visual perspective taking, seeing leads to knowing, action based knowledge, false belief), and empathy.
The Autism Yar program is a 42-session individual or group-based intervention for children with autism. Due to the COVID-19 pandemic, the intervention will be carried out online by one of the researchers, who will provide training to intervention groups. The online format as a group will be held during 45 sessions (3 days a week) for parents of autistic children. In each online group, there will be about 25 people (Table 1).
Ten sessions (3,6,9,18,21,24,27,30,33,36,39, 42) out of the total sessions will be dedicated to answering parents’ questions. Also, the therapist will do the exercises in the presence of the parents, with one of the children chosen as a model so that they can be trained.
Compensatory cognitive intervention
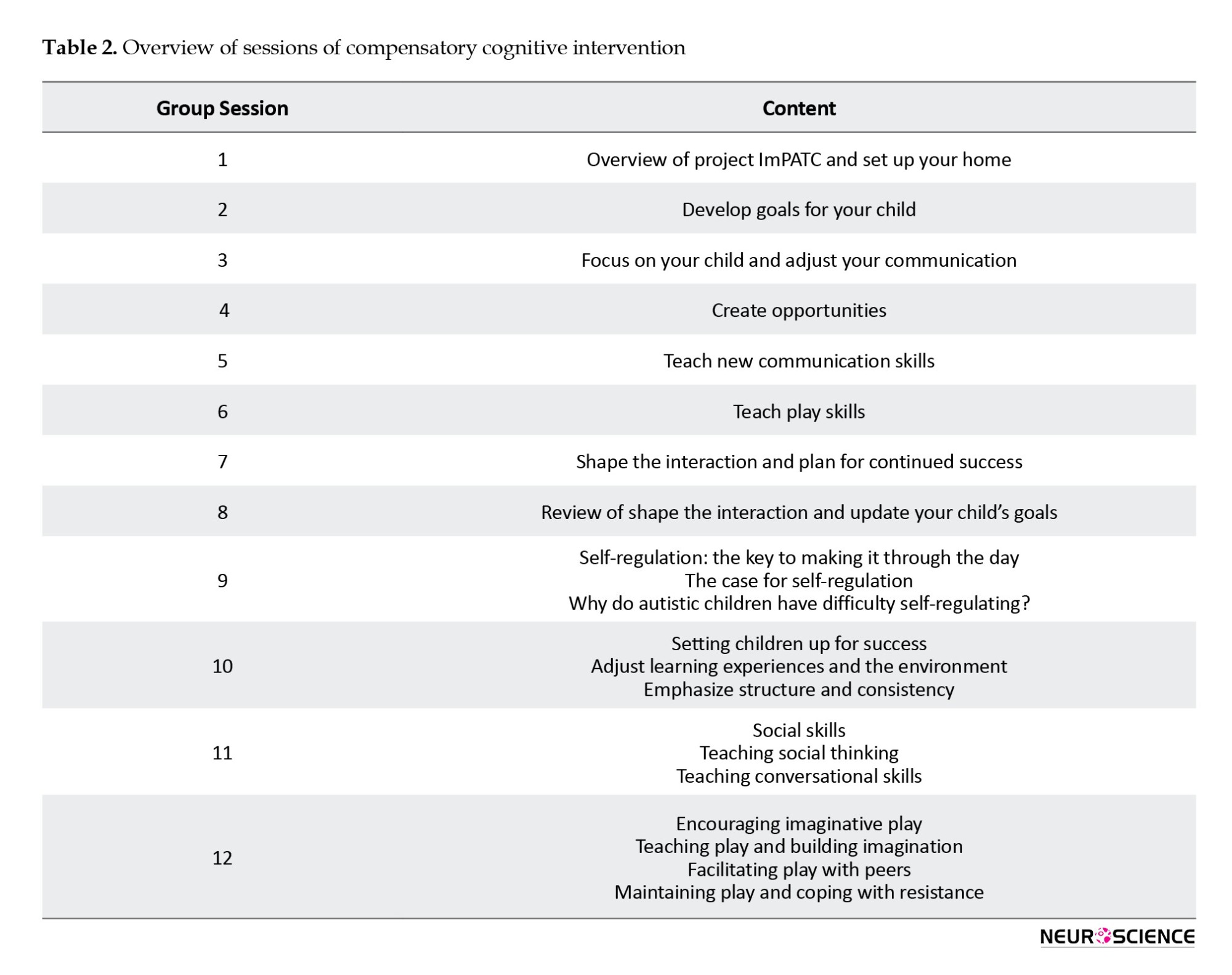
Compensatory cognitive intervention is based on parent education programs (PEP) and Project ImPACT (improving parents as communication teachers). PEP and Project ImPACT focus on the core symptom areas of ASD (such as behavioral difficulties, socialization, and communication). This program will be conducted and managed by a psychologist (a research team member) consisting of 12 (60-90 minutes) core sessions. The structured PEP sessions can be administered either individually or in groups to the parent using direct strategies, role play, filling out the daily activity schedule, video examples, and homework assignments. Parents are instructed on the underlying causes of autism disorder, the behavioral problems, how to improve the child’s impaired social and cognitive functions, and also behavior management skills. Ingersoll and Dvortcsak detail the intervention strategies and training programs for parents (Ingersoll & Wainer, 2013). Furthermore, during the sessions, the parents will be taught about using positive behavior support techniques to manage maladaptive behaviors and support the improvement of their child’s communication skills, play skills, and social functioning (Table 2) (Brereton & Tonge, 2005).
Hybrid cognitive intervention (compensatory cognitive intervention and remediation cognitive intervention)
This group of children will receive a combination of the Autism Yar program, parent education programs (PEP), and Project ImPACT over 14 weeks (4 days a week). Participants will receive the Autism Yar program 3 days a week, and the PEP will be received one day per week.
Data analysis
Before analysis, the normality of the raw data will be tested for all key variables. The primary and secondary outcomes will be analyzed using repeated measures analysis of variance (ANOVA) and mixed models as the primary design. Multiple imputations will be used for missing observations at post-test, 1-month, and 3-month follow-up. Pre-test differences in demographic characteristics (age, gender, total IQ, verbal IQ, performance IQ, parental education, and parental age) will be investigated with the chi-square tests and ANOVA. Both within (changes within-person across time) and between-subject (changes between persons in the intervention condition versus the control conditions) impacts will be investigated to determine the efficacy of the remediation and compensatory cognitive intervention. The within-subject variable “time” has four levels: T0 (pre-test), T1 (post-test), T2 (1-month follow-up), and T3 (3-month follow-up). The between-subject variable “condition” has two levels: Intervention conditions and control conditions. The eta square statistic (ŋ2) will be computed to estimate the effect size and recognize the practical significance of the results. Secondary outcomes are investigated similarly to the primary outcomes analysis. Statistical analyses were performed using SPSS software, version 22, and the two-sided P was set at 0.05.
3. Discussion
This trial aims to determine the effectiveness of an Autism Yar rehabilitation program for improving EFs and TOM skills in preschoolers with ASD. The Autism Yar can also be used as an educational and rehabilitation tool for teachers and parents by providing them with strategies to create regular and continuous learning opportunities for their children daily at home and school. Overall, the Autism Yar can intensify the positive impact of any developmental, social, and behavioral program for the treatment of ASD children (Fisher & Happe, 2005; Beeger et al., 2015).
The results of this trial will provide evidence to assess the feasibility of parents becoming therapists for their children with ASD through a rigorous yet pragmatic evaluation process. It will also provide evidence for the effectiveness of the Autism Yar program in improving trajectories for children with autism at school age (Beeger et al., 2015).
The strengths of our current trial include its multicenter, randomization, double-blinded, treatment-as-usual to control group, parallel-group trial for the comprehensive evaluation and effectiveness of a dimensional rehabilitation program in preschoolers with autism. Another strength is using multiple outcome assessment tools to obtain information from various reporters.
Three potential limitations of the present trial should be mentioned. First, trained parents will do the intervention. To confirm the rehabilitation program’s effectiveness and generalizability, the training teachers implemented should be evaluated. Second, it will not address whether the rehabilitation group’s TOM and EF gains were sustained or whether the rehabilitation program was associated with greater academic achievement and school readiness at the end of kindergarten and grade 1. It is necessary to focus future studies on the effectiveness of TOM and EFs training on academic achievement and social communication.
Third, although having an active control group is better than an inactive control group, the number of intervention sessions in the active control group (12 sessions) is not the same as the intervention groups (one received 42 sessions and the other received 54 sessions). Therefore, the improvement in performance and changes in brain activity in the intervention groups are probably partially explained by the difference in the amount of intervention between the three groups. So, the groups should receive the same intervention sessions in future studies.
Ethical Considerations
Compliance with ethical guidelines
The study protocol was approved by the Human Research Ethics Committee of the Institute of Cognitive Science Studies and Institutional Research Ethics Committee (Code: IR.UT.IRICSS.REC.1399.011). This study was also registered by the Iranian Registry of Clinical Trials (IRCT) (Code: 20210619051618N1).
Funding
This study has received funding from the Cognitive Science and Technologies Council for conducting parenting workshops, designing the trial, collecting, analyzing, and interpreting data, and developing and designing the Autism Yar rehabilitation program (Project Grant No.: 9598).
Authors' contributions
Conceptualization: Fateme Abadi, Alireza Moradi and Hadi Zarafshan; The trial design: All Authors; Methodolgy: Fateme Abadi, Meysam Sadeghi, Hadi Zarafshan and Mohamadreza Mohammadi; Data collection: Fateme abadi; Data analysis: Fateme Abadi and Meysam Sadeghi; Writing the original draft: Fateme Abadi, Alireza Moradi and Hadi Zarafshan; Review and editing: Fateme abadi and Alireza Moradi; Funding administration: Fateme Abadi and Alireza Moradi; Supervision: Alireza Moradi and Hadi Zarafshan.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the rehabilitation centers for referring their patients to the principal researcher in this study.
References
Abadi, F., Moradi, A., Zarafshan, H., Sadeghi, M., & Mohamadi, M. (2022). [Social cognition dysfunction in children with high functioning autism disorder: Evaluation, developing program based on remediation and compensation strategies and study on its effectiveness on theory of mind ability and executive function (Persian)].Tehran: Institute for Cognitive Science Studies.
Alvares, G. A., Bebbington, K., Cleary, D., Evans, K., Glasson, E. J., & Maybery, M. T., et al. (2020). The misnomer of ‘high functioning autism’: Intelligence is an imprecise predictor of functional abilities at diagnosis. Autism, 24(1), 221-232. [DOI:10.1177/1362361319852831] [PMID]
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders, 5th, Edn. Virginia: American Psychiatric Association. [DOI:10.1176/appi.books.9780890425596]
Baron-Cohen, S., Leslie, A. M., & Frith, U. (1985). Does the autistic child have a “theory of mind”? Cognition, 21(1), 37-46. [DOI:10.1016/0010-0277(85)90022-8] [PMID]
Begeer, S., Gevers, C., Clifford, P., Verhoeve, M., Kat, K., & Hoddenbach, E., et al. (2011). Theory of mind training in children with autism: A randomized controlled trial. Journal of Autism and Developmental Disorders, 41(8), 997-1006. [DOI:10.1007/s10803-010-1121-9] [PMID]
Begeer, S., Howlin, P., Hoddenbach, E., Clauser, C., Lindauer, R., & Clifford, P., et al. (2015). Effects and moderators of a short theory of mind intervention for children with autism spectrum disorder: A randomized controlled trial. Autism Research, 8(6), 738-748. [DOI:10.1002/aur.1489] [PMID]
Best, J. R., Miller, P. H., & Naglieri, J. A. (2011). Relations between executive function and academic achievement from ages 5 to 17 in a large, representative national sample. Learning and Individual Differences, 21(4), 327-336. [DOI:10.1016/j.lindif.2011.01.007] [PMID]
Blijd-Hoogewys, E. M., van Geert, P. L., Serra, M., & Minderaa, R. B. (2008). Measuring theory of mind in children. Psychometric properties of the ToM Storybooks. Journal of Autism and Developmental Disorders, 38(10), 1907-1930. [DOI:10.1007/s10803-008-0585-3] [PMID]
Brereton, A. V., & Tonge, B. J. (2005). Preschoolers with autism: An education and skills training programme for parents: Manual for clinicians. London: Jessica Kingsley Publishers. [Link]
Caputi, M., Cugnata, F., & Brombin, C. (2021). Theory of mind and loneliness: Effects of a conversation‐based training at school. International Journal of Psychology, 56(2), 257-265. [DOI:10.1002/ijop.12707] [PMID]
Carlson, S. M. (2005). Developmentally sensitive measures of executive function in preschool children. Developmental Neuropsychology, 28(2), 595-616. [DOI:10.1207/s15326942dn2802_3] [PMID]
Carlson, S. M., Claxton, L. J., & Moses, L. J. (2015). The relation between executive function and theory of mind is more than skin deep. Journal of Cognition and Development, 16(1), 186-197. [DOI:10.1080/15248372.2013.824883]
Carlson, S. M., Mandell, D. J., & Williams, L. (2004). Executive function and theory of mind: stability and prediction from ages 2 to 3. Developmental Psychology, 40(6), 1105–1122.[DOI:10.1037/0012-1649.40.6.1105] [PMID]
Carlson, S. M., Moses, L. J., & Breton, C. (2002). How specific is the relation between executive function and theory of mind? Contributions of inhibitory control and working memory. Infant and Child Development, 11(2), 73-92. [DOI:10.1002/icd.298]
Cicerone, K. D., Langenbahn, D. M., Braden, C., Malec, J. F., Kalmar, K., & Fraas, M., et al. (2011). Evidence-based cognitive rehabilitation: updated review of the literature from 2003 through 2008. Archives of Physical Medicine and Rehabilitation, 92(4), 519-530. [DOI:10.1016/j.apmr.2010.11.015] [PMID]
de Veld, D. M. J., Howlin, P., Hoddenbach, E., Mulder, F., Wolf, I., & Koot, H. M., et al. (2017). Moderating effects of parental characteristics on the effectiveness of a theory of mind training for children with autism: A randomized controlled trial. Journal of Autism and Developmental Disorders, 47(7), 1987-1997. [DOI:10.1007/s10803-017-3117-1] [PMID]
de Vries, M., Prins, P. J., Schmand, B. A., & Geurts, H. M. (2015). Working memory and cognitive flexibility‐training for children with an autism spectrum disorder: A randomized controlled trial. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 56(5), 566–576. [DOI:10.1111/jcpp.12324] [PMID]
Devine, R. T., White, N., Ensor, R., & Hughes, C. (2016). Theory of mind in middle childhood: Longitudinal associations with executive function and social competence. Developmental Psychology, 52(5), 758-771. [DOI:10.1037/dev0000105] [PMID]
Diamond, A., & Lee, K. (2011). Interventions shown to aid executive function development in children 4 to 12 years old. Science, 333(6045), 959-964. [DOI:10.1126%2Fscience.1204529] [PMID]
Espy, K. A. (1997). The Shape School: Assessing executive function in preschool children. Developmental Neuropsychology, 13(4), 495-499. [DOI:10.1080/87565649709540690]
Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175-191. [DOI:10.3758/BF03193146] [PMID]
Fisher, N., & Happé, F. (2005). A training study of theory of mind and executive function in children with autistic spectrum disorders. Journal of Autism and Developmental Disorders, 35(6), 757-771. [DOI:10.1007/s10803-005-0022-9] [PMID]
Gibb, R., Coelho, L., Van Rootselaar, N. A., Halliwell, C., MacKinnon, M., & Plomp, I., et al. (2021). Promoting executive function skills in preschoolers using a play-based program. Frontiers in Psychology, 12, 720225. [DOI:10.3389/fpsyg.2021.720225] [PMID]
Gioia, G. A., Isquith, P. K., Guy, S. C., & Kenworthy, L. (2000).Test review behavior rating inventory of executive function. Child Neuropsychology, 6(3), 235-238. [Link]
Gulsrud, A. C., Kasari, C., Freeman, S., & Paparella, T. (2007). Children with autism’s response to novel stimuli while participating in interventions targeting joint attention or symbolic play skills. Autism, 11(6), 535-546. [DOI:10.1177/1362361307083255] [PMID]
Hoddenbach, E., Koot, H. M., Clifford, P., Gevers, C., Clauser, C., & Boer, F., et al. (2012). Individual differences in the efficacy of a short theory of mind intervention for children with autism spectrum disorder: A randomized controlled trial. Trials, 13, 206. [DOI:10.1186/1745-6215-13-206] [PMID]
Horn, G. J., & Lewis, F. D. (2014). A model of care for neurological rehabilitation. Journal of Nurse Life Care Planning, 14(3), 681-692. [Link]
Ingersoll, B., & Wainer, A. (2013). Initial efficacy of Project ImPACT: A parent-mediated social communication intervention for young children with ASD. Journal of Autism and Developmental Disorders, 43(12), 2943-2952. [DOI:10.1007/s10803-013-1840-9] [PMID]
Joekar, S., Amiri, S., Joekar, S., Birashk, B., & Aghebati, A. (2017). Effectiveness of a visual attention training program on the reduction of ADHD symptoms in preschool children at risk for ADHD in Isfahan: A pilot study. Iranian Journal of Psychiatry and Behavioral Sciences, 11(4), e7862. [DOI:10.5812/ijpbs.7862]
Kenworthy, L., Anthony, L. G., Naiman, D. Q., Cannon, L., Wills, M. C., & Luong‐Tran, C., et al. (2014). Randomized controlled effectiveness trial of executive function intervention for children on the autism spectrum. Journal of Child Psychology and Psychiatry, 55(4), 374-383. [DOI:10.1111/jcpp.12161] [PMID]
Kleim, J. A., & Jones, T. A. (2008). Principles of experience-dependent neural plasticity: Implications for rehabilitation after brain damage. Journal of Speech, Language, and Hearing Research: JSLHR, 51(1), S225–S239. [DOI:10.1044/1092-4388(2008/018)] [PMID]
Leslie, A. M. (1987). Pretense and representation: The origins of” theory of mind.”. Psychological Review, 94(4), 412-426. [DOI:10.1037/0033-295X.94.4.412]
Macoun, S. J., Schneider, I., Bedir, B., Sheehan, J., & Sung, A. (2021). Pilot study of an attention and executive function cognitive intervention in children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 51(8), 2600-2610. [DOI:10.1007/s10803-020-04723-w] [PMID]
Memari, A. H., Shayestehfar, M., Mirfazeli, F. S., Rashidi, T., Ghanouni, P., & Hafizi, S. (2013). Cross-cultural adaptation, reliability, and validity of the autism treatment evaluation checklist in Persian. Iranian Journal of Pediatrics, 23(3), 269-275. [PMID]
Mishra, J., & Gazzaley, A. (2014). Harnessing the neuroplastic potential of the human brain & the future of cognitive rehabilitation. Frontiers in Human Neuroscience, 8, 218. [DOI:10.3389/fnhum.2014.00218]
Ozonoff, S., & Miller, J. N. (1995). Teaching theory of mind: A new approach to social skills training for individuals with autism. Journal of Autism and Developmental Disorders, 25(4), 415-433. [DOI:10.1007/bf02179376] [PMID]
Partanen, P., Jansson, B., Lisspers, J., & Sundin, Ö. (2015). Metacognitive strategy training adds to the effects of working memory training in children with special educational needs. International Journal of Psychological Studies, 7(3), 130-140. [DOI:10.5539/ijps.v7n3p130]
Pasqualotto, A., Mazzoni, N., Bentenuto, A., Mulè, A., Benso, F., & Venuti, P. (2021). Effects of cognitive training programs on executive function in children and adolescents with Autism Spectrum Disorder: A systematic review. Brain Sciences, 11(10), 1280. [DOI:10.3390/brainsci11101280] [PMID]
Perner, J., & Lang, B. (1999). Development of theory of mind and executive control. Trends in Cognitive Sciences, 3(9), 337-344. [DOI:10.1016/s1364-6613(99)01362-5] [PMID]
Re, A. M., Capodieci, A., & Cornoldi, C. (2015). Effect of training focused on executive functions (attention, inhibition, and working memory) in preschoolers exhibiting ADHD symptoms. Frontiers in Psychology, 6, 1161. [DOI:10.3389%2Ffpsyg.2015.01161] [PMID]
Rossignoli-Palomeque, T., Quiros-Godoy, M., Perez-Hernandez, E., & González-Marqués, J. (2019). Schoolchildren’s compensatory strategies and skills in relation to attention and executive function app training. Frontiers in Psychology, 10, 2332. [DOI:10.3389%2Ffpsyg.2019.02332] [PMID]
Scionti, N., Cavallero, M., Zogmaister, C., & Marzocchi, G. M. (2020). Is cognitive training effective for improving executive functions in preschoolers? A systematic review and meta-analysis. Frontiers in Psychology, 10, 2812. [DOI:10.3389/fpsyg.2019.02812] [PMID]
Shahim S. (2006). Wechsler Intelligence Scale for children revised: The agenda and norms. Shiraz: Shiraz University press.
Sohlberg, M. M., Avery, J., Kennedy, M., Ylvisaker, M., Coelho, C., & Turkstra, L., et al. (2003). Practice guidelines for direct attention training. Journal of Medical Speech Language Pathology, 11(3), xix--xxxi. [Link]
Spaniol, M. M., Mevorach, C., Shalev, L., Teixeira, M. C. T. V., Lowenthal, R., & de Paula, C. S. (2021). Attention training in children with autism spectrum disorder improves academic performance: A double‐blind pilot application of the computerized progressive attentional training program. Autism Research, 14(8), 1769-1776. [DOI:10.1002/aur.2566] [PMID]
Steerneman, P., Jackson, S., Pelzer, H., & Muris, P. (1996). Children with social handicaps: An intervention programme using a theory of mind approach. Clinical Child Psychology and Psychiatry, 1(2), 251-263. [DOI:10.1177%2F1359104596012006]
Volckaert, A. M. S., & Noël, M. P. (2015). Training executive function in preschoolers reduce externalizing behaviors. Trends in Neuroscience and Education, 4(1-2), 37-47. [DOI:10.1016/j.tine.2015.02.001]
Wechsler, D., & Kort, W. (2005). WISC-III NL: Wechsler Intelligence Scale for Children. Texas: Harcourt Assessment.
Wellman, H. M. (2002). Understanding the psychological world: Developing a theory of mind. In U. Goswami (Ed.), Blackwell handbook of childhood cognitive development (pp. 167-187). Oxford: Blackwell Publishers Ltd. [DOI:10.1002/9780470996652.ch8]
Wellman, H. M., & Liu, D. (2004). Scaling of theory‐of‐mind tasks. Child Development, 75(2), 523-541. [DOI:10.1111/j.1467-8624.2004.00691.x] [PMID]
Wellman, H. M., Baron-Cohen, S., Caswell, R., Gomez, J. C., Swettenham, J., & Toye, E., et al. (2002). Thought-bubbles help children with autism acquire an alternative to a theory of mind. Autism, 6(4), 343-363. [DOI:10.1177/1362361302006004003] [PMID]
Wykes, T., Huddy, V., Cellard, C., McGurk, S. R., & Czobor, P. (2011). A meta-analysis of cognitive remediation for schizophrenia: Methodology and effect sizes. The American Journal of Psychiatry, 168(5), 472–485. [DOI:10.1176/appi.ajp.2010.10060855] [PMID]
Ylvisaker, M., Turkstra, L., Coehlo, C., Yorkston, K., Kennedy, M., & Sohlberg, M. M., et al. (2007). Behavioural interventions for children and adults with behaviour disorders after TBI: A systematic review of the evidence. Brain Injury, 21(8), 769-805. [DOI:10.1080/02699050701482470] [PMID]
Zelazo, P. D. (2015). Executive function: Reflection, iterative reprocessing, complexity, and the developing brain. Developmental Review, 38, 55-68. [DOI:10.1016/j.dr.2015.07.001]
Type of Study: Methodological Notes |
Subject:
Clinical Neuroscience
Received: 2022/12/3 | Accepted: 2023/03/15 | Published: 2024/11/1
Received: 2022/12/3 | Accepted: 2023/03/15 | Published: 2024/11/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
