

Volume 16 - Special Issue on Cognitive Sciences
BCN 2025, 16 - Special Issue on Cognitive Sciences: 219-232 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Niroumand Sarvandani M, Garmabi B, Asadi M, Ghazvini H, Rafaiee R, Kalalian Moghaddam H. Impact of Circadian Rhythm Disturbance and Chronotype on Medical Students' Mental State. BCN 2025; 16 (S1) :219-232
URL: http://bcn.iums.ac.ir/article-1-2502-en.html
URL: http://bcn.iums.ac.ir/article-1-2502-en.html
Mohammad Niroumand Sarvandani1 

 , Behzad Garmabi2 , Masoud Asadi3 , Hamed Ghazvini4 , Raheleh Rafaiee5 , Hamid Kalalian Moghaddam *6
, Behzad Garmabi2 , Masoud Asadi3 , Hamed Ghazvini4 , Raheleh Rafaiee5 , Hamid Kalalian Moghaddam *6
, Behzad Garmabi2 , Masoud Asadi3 , Hamed Ghazvini4 , Raheleh Rafaiee5 , Hamid Kalalian Moghaddam *6
1- Student Research Committee, School of Medicine, Shahroud University of Medical Sciences, Shahroud, Iran.
2- School of Medicine, Shahroud University of Medical Sciences, Shahroud, Iran.
3- Department of Psychology, Faculty of Humanities, Arak University, Arak, Iran.
4- Psychiatry and Behavioral Sciences Research Center, Addiction Institute, Mazandaran University of Medical Sciences, Sari, Iran.
5- Department of Neuroscience, School of Advanced Technologies in Medicine, Mazandaran University of Medical Sciences, Sari, Iran.
6- Department of Addiction Studies, School of Medicine, Shahroud University of Medical Sciences, Shahroud, Iran.
2- School of Medicine, Shahroud University of Medical Sciences, Shahroud, Iran.
3- Department of Psychology, Faculty of Humanities, Arak University, Arak, Iran.
4- Psychiatry and Behavioral Sciences Research Center, Addiction Institute, Mazandaran University of Medical Sciences, Sari, Iran.
5- Department of Neuroscience, School of Advanced Technologies in Medicine, Mazandaran University of Medical Sciences, Sari, Iran.
6- Department of Addiction Studies, School of Medicine, Shahroud University of Medical Sciences, Shahroud, Iran.
Keywords: Anxiety, Circadian rhythm, Depression, Stress disorders, Substance-related disorders, Chronobiology, Boredom
Full-Text [PDF 1500 kb]
| Abstract (HTML)
Full-Text:
1. Introduction
Living organisms exhibit various cyclic physiological changes over the day and night cycle (Kim & Kim, 2019; Patke et al., 2020). In most animals and humans, the sleep-wake rhythm is the most obvious diurnal rhythm (Rivkees, 2007). Misalignment of circadian rhythms may result from a mistimed light-dark cycle and feeding time, or there may even be misalignment between the peripheral and central rhythms (Lewis et al., 2020; West et al., 2017). The medical literature reports that misalignment has intense effects on processes that influence the risk of cardiovascular disease, as well as metabolic and neuropsychiatric conditions (Hower et al., 2018; Moreno et al., 2019; Walker et al, 2020). Sleep disturbance is one of the most immediate and significant consequences of the misalignment of the sleep-wake cycle with the biological night (Ingram, 2020). Circadian variability affects wakefulness, feeding behavior, metabolic function, and mood differently (Parkar et al., 2019; Poggiogalle et al., 2018; Zaki et al., 2018).
People have been divided into chronotype groups since the beginning of the 20th century (Becker et al., 2016). Chronotypes can generally be categorized into three types: Morning types, evening types, and non-types, which differ according to several behavioral, psychological, and biological variables, including usual eating times, appetite, mood, performance, and alertness (Kim & Kim, 2019; Kivelä et al., 2018). Morning types start their activities earlier in the morning, while evening types are more efficient later in the day (Matchock & Mordkoff, 2009). Morning types are tested in the morning, and evening types are tested in the evening. They respond more quickly to tasks that measure their reaction time (Lara et al., 2014). Shift workers usually undergo circadian misalignment, which appears when the feeding and sleep-wake cycles are desynchronized with the temporal framework organized by the internal biological clock. People differ considerably in their tolerance to shift work depending on their chronotype. Several studies have highlighted that evening types are a risk factor for depressive symptoms and the onset of depressive disorder in young people (Lotti et al., 2021). In studies that investigated the relationship between chronotype in university students, detrimental effects of sleep deprivation due to studying included decreased cognitive performance, lower motivation, increased aggression, increased depression, daytime sleepiness, and addictive behaviors (Montaruli et al., 2019; Van den Berg et al., 2018). Nursing and medical studies are also related to making up for sleep deprivation, circadian disruption, and missed weekend sleep on weekends or days off (López‐Soto et al., 2019; Sun et al., 2019).
It has been demonstrated that the circadian misalignment affects essential systems in the body. The link between misalignment of circadian rhythms, neurocognitive dysfunction, and substance use disorder may lie in the changed function of neural circuits underlying cognitive processing, reward, and impulse control (Hasler et al., 2015; Mattis & Sehgal, 2016; Wallace, 2020). Transgenic animal models show that circadian genes (e.g. Per1, Per2, and CLOCK) in reward circuits of the brain play a role in the regulation of appetitive behavior, and both clinical and preclinical research suggests a relationship between circadian genes and reward function (Rijo-Ferreira & Takahashi, 2019). Substantial neuroimaging literature has examined the possible links between circadian rhythm shifts and alterations in neural circuitry in the human brain (DePoy et al., 2017).
Given the increasingly stressful and heavy workload of the COVID-19 pandemic, circadian disorders and resulting complications are expected to increase in some health professionals and students (Marvaldi et al., 2021). It is essential for health policymakers to constantly update their information on the health status of health professionals and its changes over time to enable accurate and timely management. Considering that there are few epidemiological studies investigating circadian disorders in medical students, the present research was conducted to fill the gap in this critical point. The current study aimed to obtain information about circadian disorders and chronotype (as a mediating variable) on resulting mental states such as impulsivity, depression, anxiety, stress, addiction potential, and boredom in students of a medical university in northeastern Iran.
2. Materials and Methods
Study design and procedures
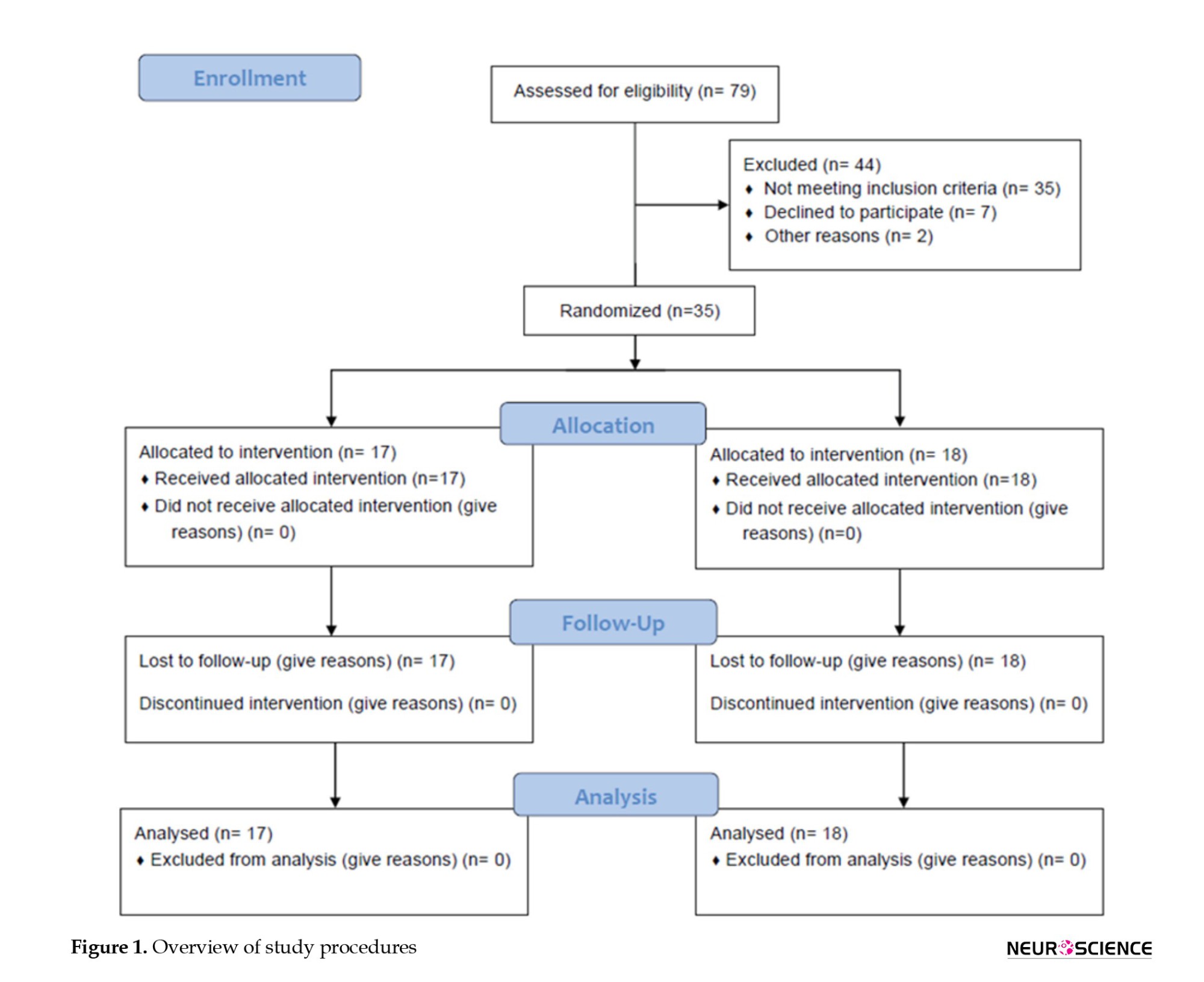
This research is a double-blind, randomized, controlled clinical trial. An overview of the study is provided in Figure 1. After written informed consent was obtained, an assistant randomly assigned subjects to the intervention or control group, and baseline data were obtained. Participants were asked to repeat the examinations at the end of the week.
Study participants
The intervention and control groups, selected from all students of Shahroud University of Medical Sciences, Shahroud City, Iran, were transferred to the experimental site in a specific dormitory for 11 days and housed in unique rooms where the light intensity is specially designed according to luxury, period and light reception time, hours of food intake. The inclusion criteria were male gender, right-handed, aged between 18 and 25 years, and regular sleep and wake rhythm in the last month (8 to 10 hours of sleep per night). The exclusion criteria were a past medical history of psychiatric illness, history of substance use, use of psychotropic drugs, a general medical disorder that endangers the subject’s health during the test, a history of brain trauma, metal bodies in the body, including platinum, fragments, or iron fragments, an irregular sleep and wake rhythm in the past month (8 to 10 hours of sleep per night), and a body mass index (BMI) greater than 30.
Randomization and blinding
To ensure the blinding of the investigators, the research coordinator carried out block randomization. Both participants and investigators are blinded to the group protocol. Participants were asked not to disclose details about their condition to their investigator to prevent unblinding. If subjects disclose their treatment, the investigator is immediately replaced by the blinded principal investigator of the project participant.
Study instruments
Reduced morningness-eveningness-questionnaire (rMEQ)
The German version of the rMEQ was applied to collect data. The rMEQ is a brief form of the morningness-eveningness questionnaire designed by Horne & Östberg, (1976). The original version contained 19 items and was rated on a Likert-type scale (Horne & Östberg, 1976). Adan & Almirall, (1991) identified a short version of this original form, which was then used in different countries, such as Iran (Adan & Almirall, 1991). rMEQ has adequate psychometric properties, good convergent and construct validity, and test re-test reliability. The scale contains 5 items linked to peak performance, preferred bedtime, time of rising, morning fatigue, and a global self-evaluation item. The Cronbach α was 0.62, and the German version was a reliable and valid measure of chronotype. Participants are classified with scores from high to low into the following types: A total rMEQ score of 18 and above as morning types, between 12 and 17 as intermediate types, and 11 and below as evening types (Adan & Almirall, 1991; Marvaldi et al., 2021).
Multidimensional state boredom scale (MSBS)
Fahlman et al., (2013) developed a MSBS as the first and full-scale measurement of state boredom (Fahlman et al., 2013). In the present study, we applied the Persian version of the MSBS, which was validated on a sample of adults by Mohseni-Ezhiyeh et al. (2017). It has a factor structure similar to the original questionnaire (i.e. 5 factors and 29 items). The Persian version of the MSBS is equivalent to the original version in terms of conceptual and linguistic features. The internal consistency of the Persian version of the MSBS was good. Its Cronbach α is 0.94 for the total score and between 0.80 and 0.89 for the subscale scores (Mohseni-Ezhiyeh & Ghamarani, 2017).
Addiction potential scale (APS)
Weed and Butcher created the APS in 1992 (Weed et al., 1992). In the current study, we used the Persian version of this scale designed by Zargar (2007). This scale contained 2 factors, 36 items, and 5 lie detector items. Most items of the first factor (the active factor) are associated with a tendency to substance use, depression, antisocial behavior, positive attitude to substance use, and sensation seeking. Most items of the second factor (the passive factor) are associated with a lack of depression and assertiveness. The criterion validity test revealed that the mentioned scale can discriminate well between substance users and non-users. The internal validity of this scale was 0.88 (Zargar et al., 2008).
Depression, anxiety, and stress scale-21 (DASS-21)
This study used data from 21 items of the depression, anxiety, and stress scale-42 (DASS-42) (i.e. the DASS-21) developed by Guillemin et al. (1993). Each of the three scales of the DASS-21 contains seven items. The items of the DASS-21 refer to the past week. Each item is scored on a 4-point Likert scale from 0 to 21. The higher the score indicated, the more severe the depression, anxiety, and stress (Asghari et al., 2008; Guillemin et al., 1993).
Barratt impulsiveness-11 (BIS-11)
The BIS-11 (11th version) was developed by Patton et al. (1995). It contains 30 items rated on a 5-point Likert scale. Twelve items are reverse-scored. It also includes three second-order parameters: Attention, motor skills, and non-planning. High scores indicate lower levels of attention, hyperactivity, and lack of planning. Its effectiveness in assessing impulsive dimensions is well established. In Iran, the norm is reduced to 25. In the present study, a 25-question form was used. The internal consistency of Persian BIS-11 is reported to be very acceptable (α=0.81) (Javid et al., 2012; Stanford et al., 2009).
Study intervention
Each participant underwent an 8-day study protocol to measure the effects of circadian misalignment on outcomes (Figure 2). One protocol applied circadian misalignment, and the other presented circadian alignment (Circadian alignment protocol, n=17; circadian misalignment protocol, n=18). On the first day of the 8-day study protocol, the subjects were accepted to the designated dormitory at ~8 AM to perform either the circadian rhythm alignment protocol or the circadian rhythm misalignment protocol (Figure 2). In the circadian alignment protocol, the subjects slept between 11:00 PM and 7:00 AM on days 1-8. In the circadian misalignment protocol, the subjects slept between 11:00 PM and 7:00 AM on days 1-3. On day 4 of the misalignment protocol, the subjects’ activation patterns were shifted by 12 hours, and this reversed cycle remained until the protocol’s end (day 8). The 12-hour shift on day 4 was made by an 8-hour wake episode and a 4-hour sleep opportunity, and the ratio of sleep opportunity to wake (1:2) remained the same in the adaptation and circadian alignment and misalignment protocols. Figure 2 shows the right conditions during the protocols.

Study outcomes
The outcome of this study is the change from baseline in scales measured by MSBS, APS, DASS-21, and BIS -11 by the end of the intervention.
Statistical analysis
Sample size calculation
The required sample size, according to Z(1-α)=1.96, power=0.9, α=0.05, d=0.8, and considering the rate of loss of 10% was calculated 34 (17 people in each group). Sample size was measured using the formula for randomized controlled trial studies as follows:
Efficacy analysis
All analyses were conducted in SPSS software, version 25. The two study groups’ pre-test and post-test Mean±SD were calculated. In preliminary analyses, we examined the pre-test result in two groups using the independent t-test (equality of means) and Levene’s test (equality of variances). We tested primary hypotheses regarding circadian misalignment effects on post-test measures using multivariate analysis of covariance (MANCOVA), Eta squared (η2), and power. We also categorized participants based on chronotype as a mediate variable within each group (circadian aligned and misaligned condition) to analyze outcomes using a one-way analysis of variance (ANOVA). We provide adjusted P to account for multiple comparisons of primary analyses using a Bonferroni post hoc test. The significance level was set at 0.05.
3. Results
Thirty-five participants were randomly assigned to circadian alignment/misalignment protocols (circadian alignment protocol, n=17; circadian misalignment protocol, n=18).
The mean age was 21.66 years (18-25 years). Thus, complete follow-up was available for 35 subjects. Figure 3 shows a consolidated standards of reporting trials (CONSORT) flowchart for the study. The obtained F value for the pre-test scores showed no significant difference between the groups at the pre-test (P>0.05).

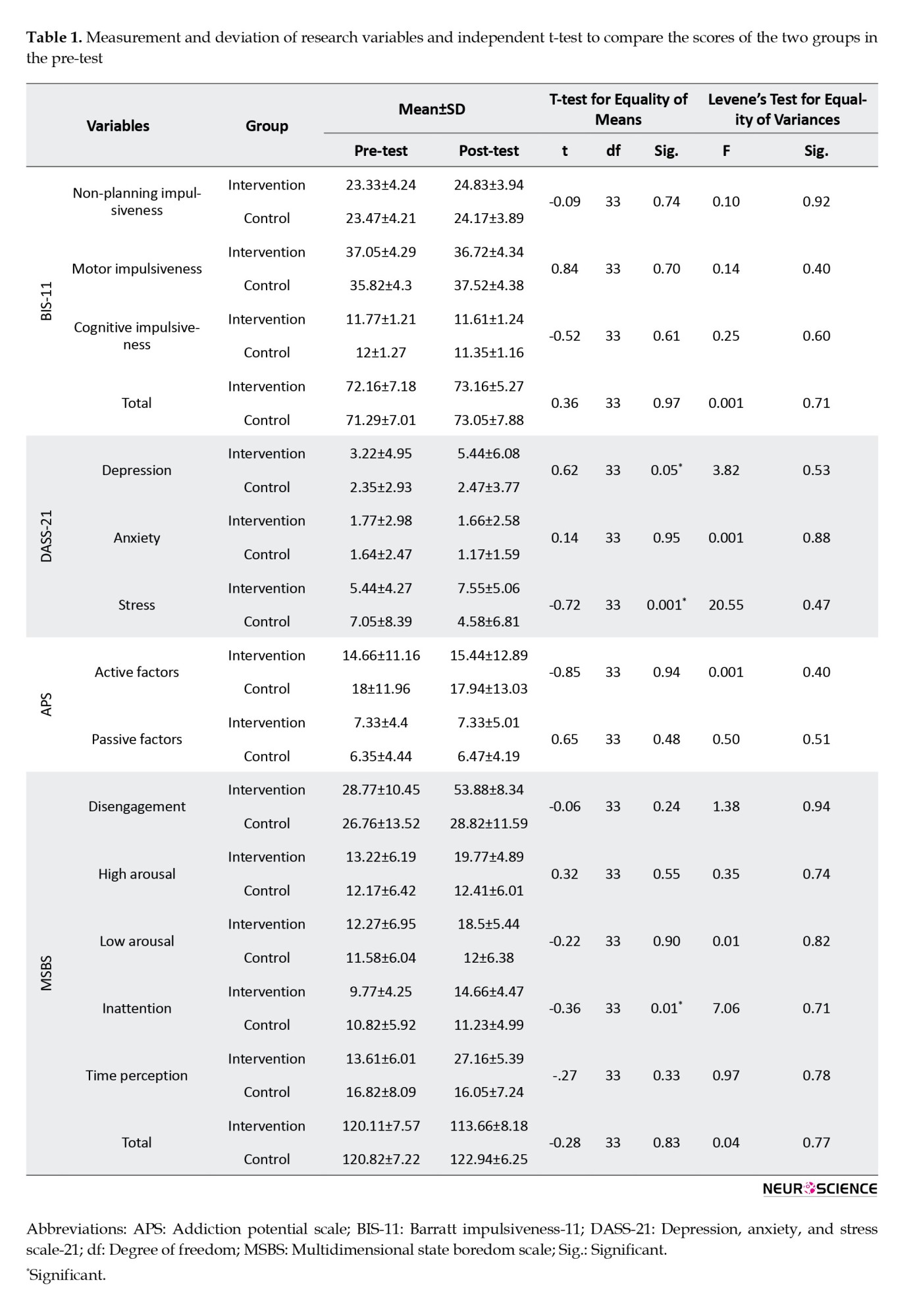
As shown in Table 1, there is a difference between the mean scores of some research variables in the two measurement phases. Box’s test of equality of covariance matrices shows that the homogeneity of the variance-covariance matrix is satisfied (Box’s M=129.73, F=1.25, df=28, P=0.087).
The result of Wilks’ lambda test in the post-test showed that the independent variable (circadian misalignment) was effective on at least one of the dependent variables in the intervention group (F=5.88, df=13.8, P=0.009, ƞ2=0.90, 1-β=0.95). Analysis of covariance was used to evaluate the effect (Table 2).
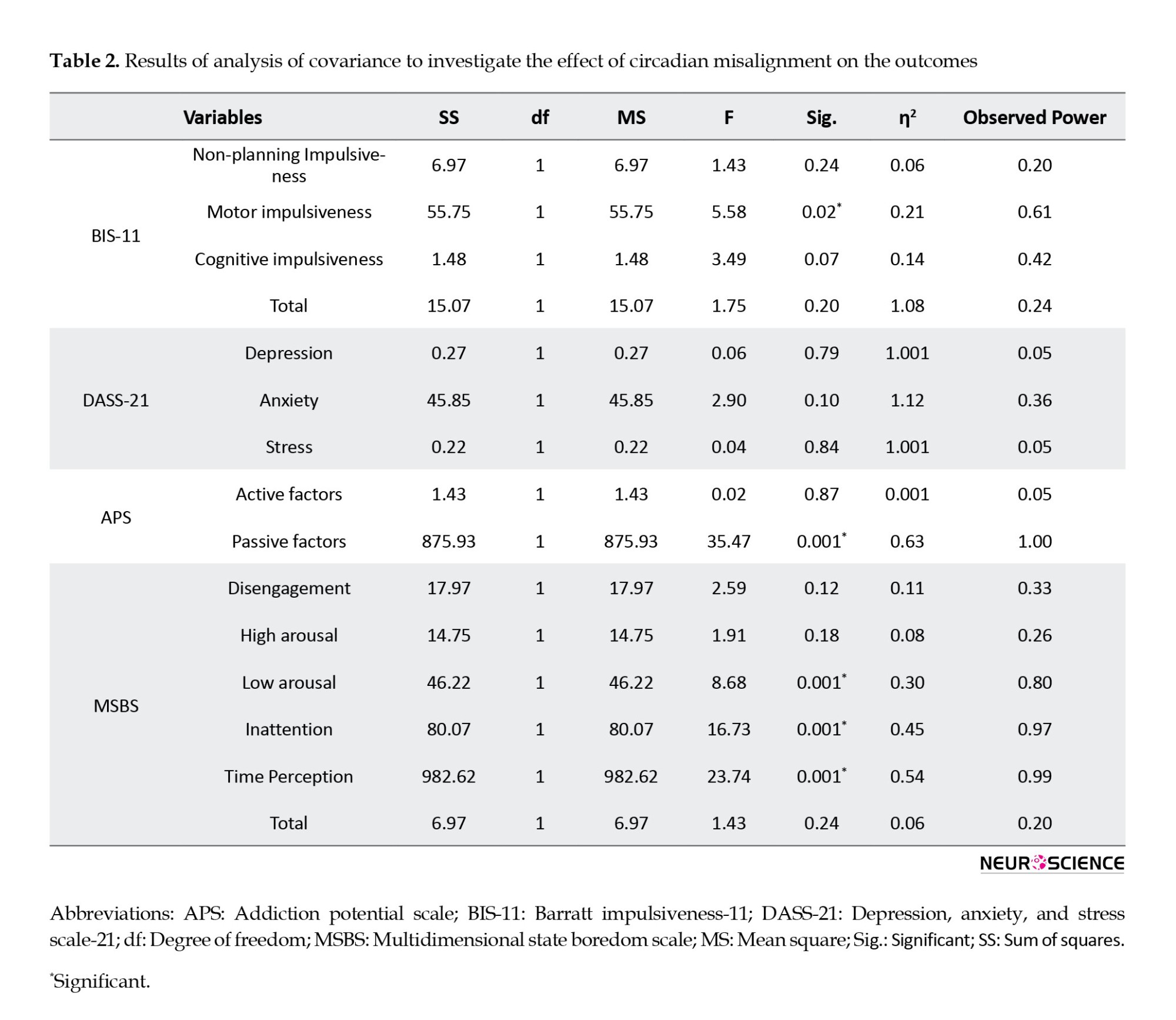
Table 2 shows that circadian misalignment was effective in motor impulsivity, passive addiction potential, low arousal, inattention, and time perception. Results of the eta-squared coefficient show that the effect of circadian misalignment on motor impulsivity, passive addiction, low arousal, inattention, and time perception was high and that among the variables, the impact on time perception was the largest.
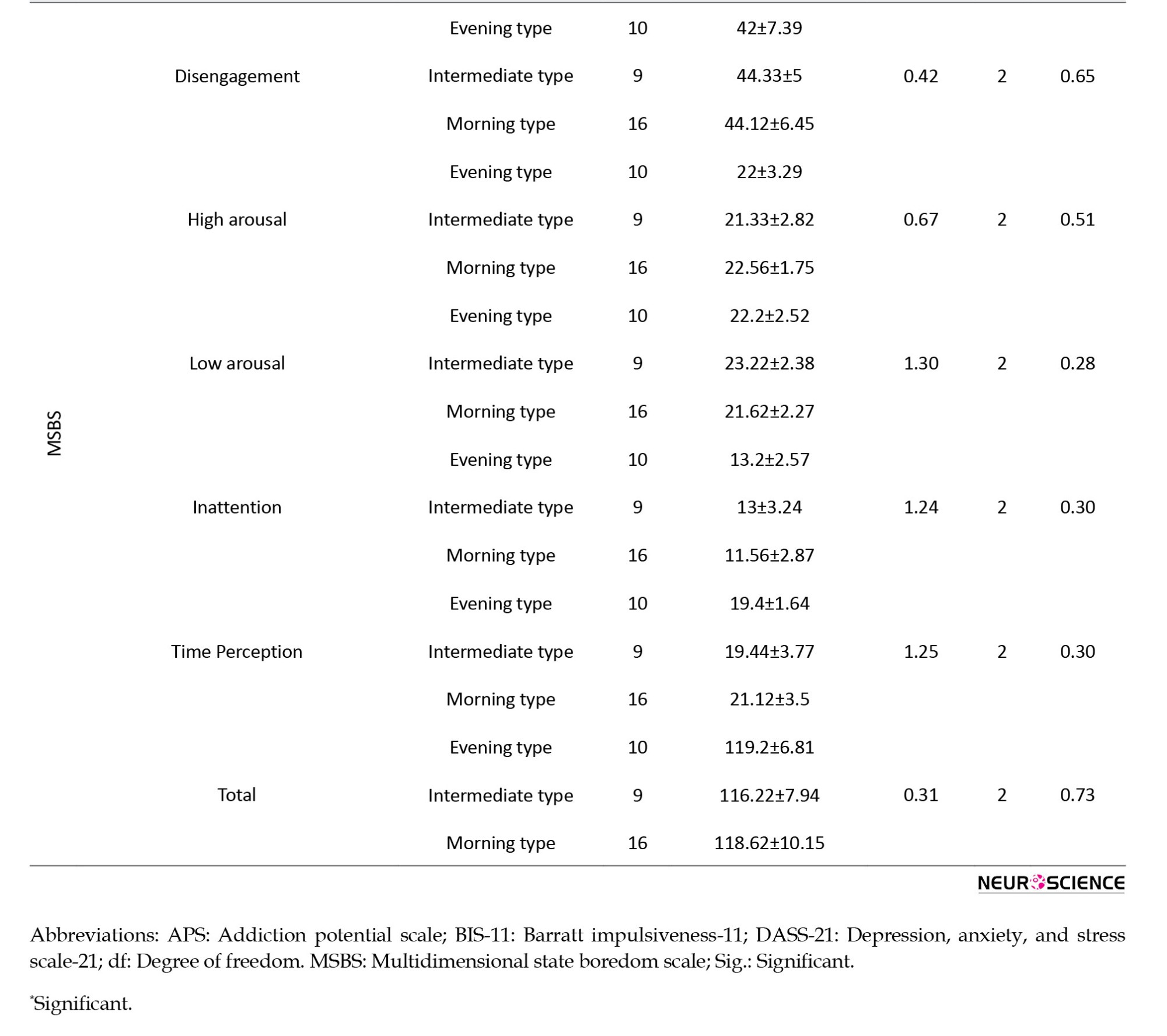
Table 3 presents a one-way ANOVA to compare research variables in groups based on chronotype (evening, intermediate, and morning types). There is a significant difference between the three groups of chronotype regarding total and non-planning impulsivity, as well as active and passive addiction potential.
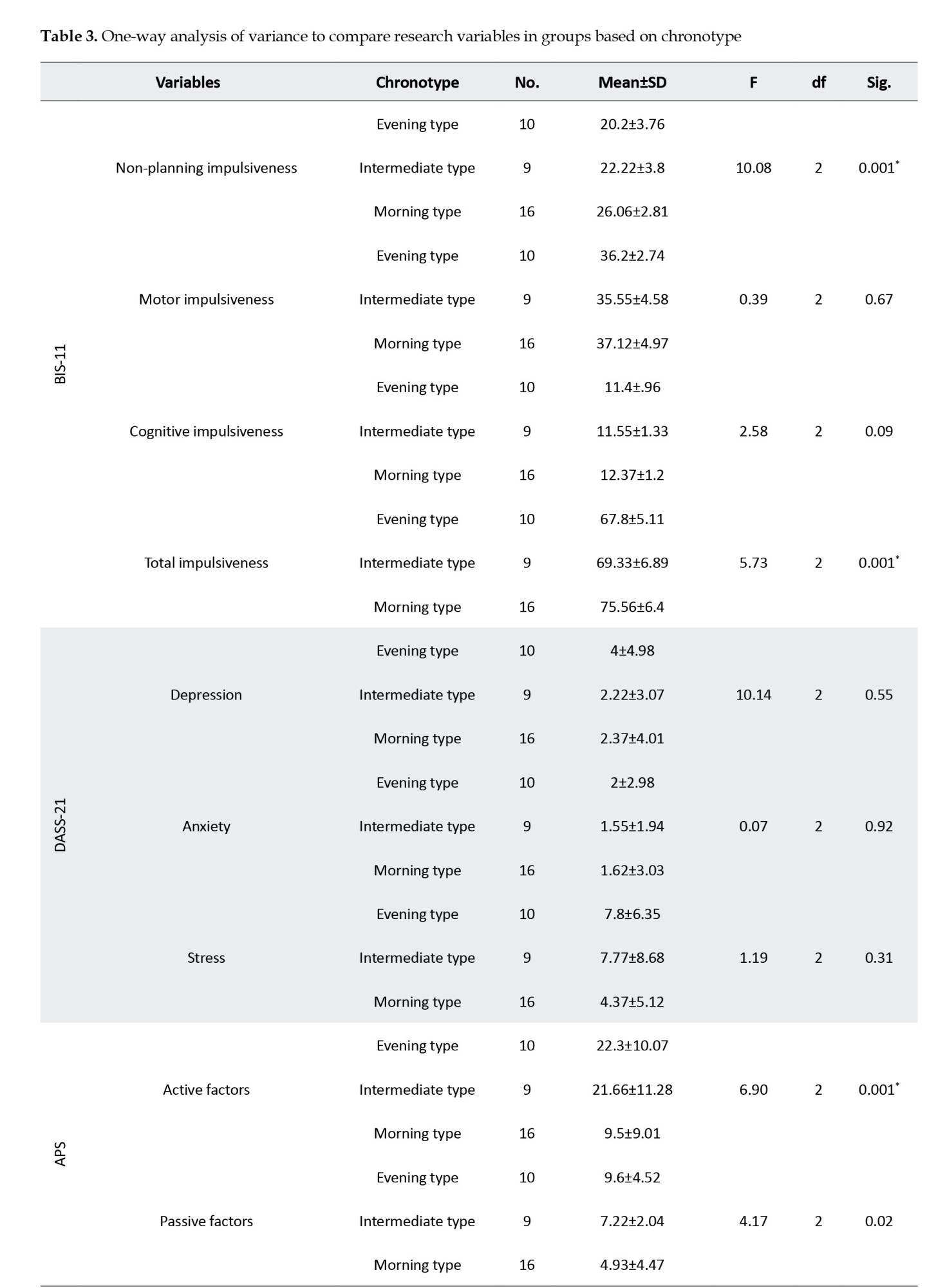
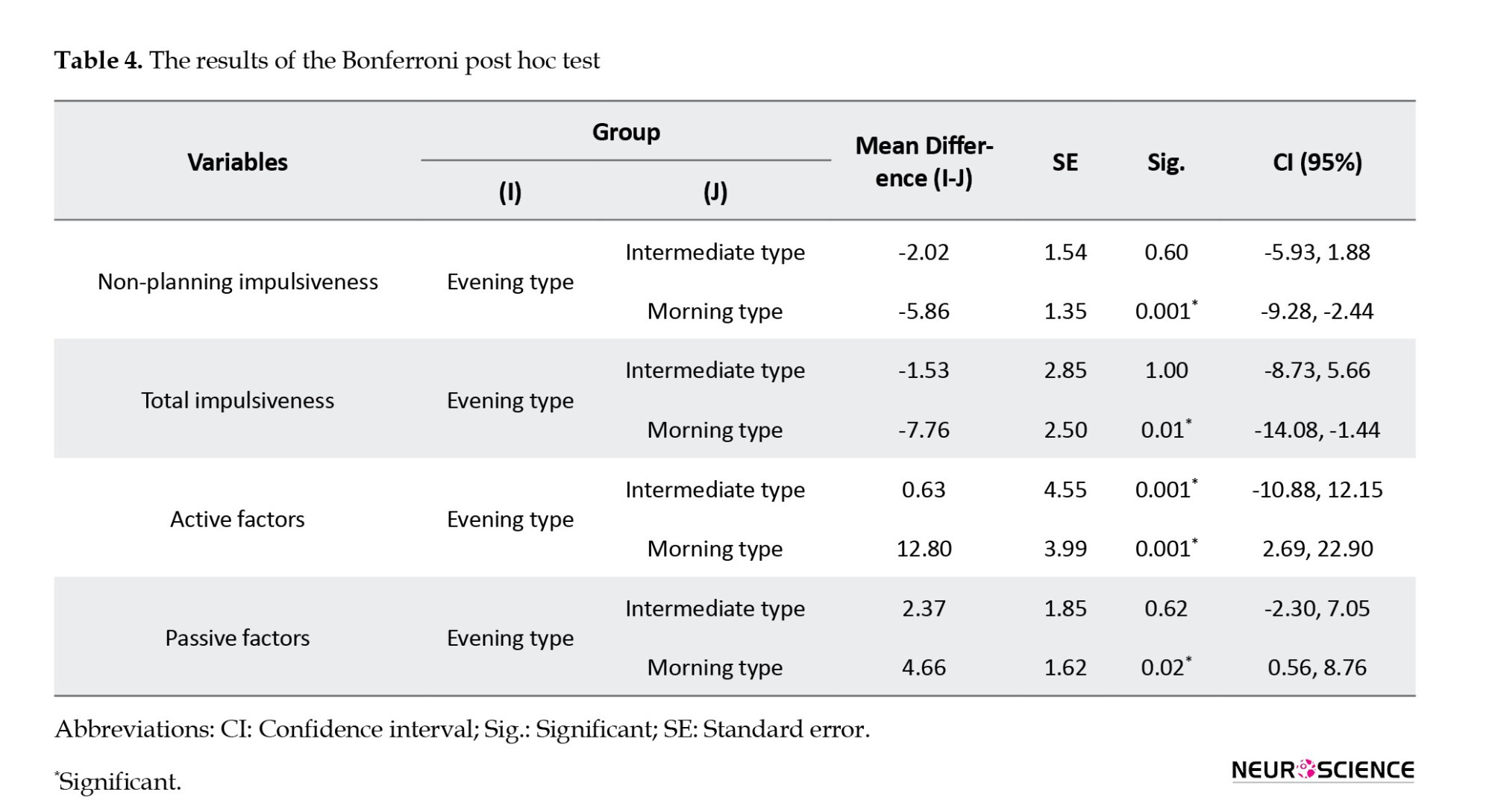
The results of the Bonferroni post hoc test to compare the mean of variables in the chronotype groups about total and non-planning impulsivity scores, active and passive addiction showed that non-planning and active addiction in persons with evening and intermediate types were significantly lower than persons with morning type. The total scores of impulsivity and passive factors of addiction potential in participants with the morning type are significantly higher than in participants with the evening type. Table 4 presents the results of the Bonferroni post hoc test.
4. Discussion
In the present study, we aimed to investigate a one-week circadian misalignment resulting from an inversion of the activation cycle (such as the feeding and sleep-wake), which is typical in shift workers and medical students based on chronotype as a mediating variable, on impulsivity, depression, anxiety, stress, addiction potential, and boredom. The major findings from the present study are as follows. First, there was a significant association between circadian misalignment and motor impulsivity, passive factors of addiction potential, low arousal, inattention, and time perception (subscales of boredom). Second, persons with circadian misalignment and a morning type showed significantly more total and non-planning impulsivity and active and passive addiction potential in comparison with other types. The outcomes of this study have important hints for health care providers. Monitoring and paying attention to the mental health of medical care providers improves the quality of health services in the community.
In accordance with the relevant literature, our results indicate that participants involved in circadian misalignment have psychological conditions compared to a healthy control group with circadian-aligned conditions (Baron & Reid, 2014; Walker et al, 2020). Our findings showed that the problems comprised impulsivity, addiction potential, and boredom. Previous studies have shown that eveningness is a risk factor for impulsivity. Another consistent finding was that having an evening-type and circadian misalignment significantly related to impulsivity and addiction potential (Hwang et al., 2016; Kang et al., 2015; Selvi et al., 2011). In a systematic review, Gillett et al. (2021) reported a significant relationship between circadian rest-activity pattern disturbance (actigraphic variables) and impulsivity and mood disorder in participants aged 12–65. Also, our results, in line with the medical literature, showed circadian misalignment prospectively related to the potential of substance use (Claudatos et al., 2019; Logan et al., 2018). It is understood that impulsiveness makes a person prone to addiction. Tamura et al. reviewed the bidirectional relationship between substance use and the circadian system. They showed each drug follows a circadian pattern and changes during the development of substance use disorder. Furthermore, the expression of the CLOCK gene is also altered with the progression of addiction in many brain regions associated with reward circuits, addictive behaviors, and relapse (Tamura et al., 2021).
Multiple types of the research reported emotions, affect, mood, motivation, especially achievement emotions (e.g. boredom and anger), have been addressed in relation to chronotype (Fabbian et al., 2016; Itzek-Greulich, Randler, & Vollmer, 2016; Kadzikowska-Wrzosek, 2020). However, no study examined the effect of circadian misalignment on boredom. The present study showed a significant relationship between circadian misalignment and boredom. On the other hand, many preclinical and clinical studies have addressed a clear link between altered circadian system on depression, anxiety and stress, which was inconsistent with our findings (Blume et al., 2019; Difrancesco et al., 2019; Kim et al., 2017; Koch et al., 2017; Landgraf et al., 2016). Chellappa et al. conducted a study in 2020. They found circadian misalignment due to simulated night shifts significantly reduced mood and well-being levels throughout days of misalignment compared to circadian alignment conditions in the non-shift workers’ group (Chellappa et al., 2020). Several research studies have shown a potential causal relationship between disturbed circadian and hypothalamic-pituitary-adrenal axis dysregulation (Nader, Chrousos, & Kino, 2010). Also, animal models show that the circadian genes Per1 and Peir2 in the nucleus accumbens regulate anxiety-related behavior (Spencer et al., 2013). One possible explanation for inconsistent findings is our small sample size.
First, the sample size was small in terms of the study limitations. Second, neuropsychological variables were measured by self-report rather than behavioral and physiological measures via actigraphy. Third, the intervention protocol in this study was the same in all three groups: Morning types, intermediate types, and evening types. On the other hand, in this study, the researchers could not find a valid protocol that could be used separately for each of these three groups. Fourth, although we could recruit female participants due to cultural constraints, it could have led to serious and time-consuming problems in implementing this project. Future researchers are recommended to repeat the present study with female participants because there are significant differences in chronotype according to gender. It is also recommended that the study be conducted using different protocols based on different chronotypes to control the testing conditions better. Our findings add to previous literature by investigating the effectiveness of the circadian system on neuropsychiatric conditions. The results of this study have important implications for clinical care providers in terms of shift work.
5. Conclusion
Alterations in diurnal profiles of activity, sleep, and feeding time, based on chronotype related to impulsiveness and boredom, and such circadian misalignment is associated with addiction potential.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Review Committee of Shahroud University of Medical Sciences, Shahroud, Iran (Code: IR.SHMU.REC.1399.170). The study was designed and carried out based on the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research established by the Iranian Registry of Clinical Trials (IRCT), Tehran, Iran (Code: 20210202050223N1). All the participants signed their informed written consent.
Funding
The present study was extracted from the PhD dissertation of Mohammad Niroumand Sarvandani, approved by the Department of Addiction Studies, School of Medicine, Shahroud University of Medical Sciences, Shahroud, Iran (No.: 838). This study was financially supported by the Research Deputy of Shahroud University of Medical Sciences, Shahroud, Iran (Grant No.: 99119).
Authors' contributions
Conceptualization: Mohammad Niroumand Sarvandani; Methodology: Raheleh Rafaiee, Hamed Ghazvini and Behzad Garmabi; Formal analysis and software: Masoud Asadi; Investigation: Mohammad Niroumand Sarvandani, and Hamed Ghazvini; Writing the original draft: Raheleh Rafaiee, and Mohammad Niroumand Sarvandani; Review and editing: Hamid Kalalian Moghaddam; Funding acquisition, resources, and supervision: Hamid Kalalian Moghaddam; Final approval: All authors.
Conflict of interest
All authors declared no conflict of interest.
Acknowledgments
The authors appreciate all the individuals who collaborated in the study.
References
Living organisms exhibit various cyclic physiological changes over the day and night cycle (Kim & Kim, 2019; Patke et al., 2020). In most animals and humans, the sleep-wake rhythm is the most obvious diurnal rhythm (Rivkees, 2007). Misalignment of circadian rhythms may result from a mistimed light-dark cycle and feeding time, or there may even be misalignment between the peripheral and central rhythms (Lewis et al., 2020; West et al., 2017). The medical literature reports that misalignment has intense effects on processes that influence the risk of cardiovascular disease, as well as metabolic and neuropsychiatric conditions (Hower et al., 2018; Moreno et al., 2019; Walker et al, 2020). Sleep disturbance is one of the most immediate and significant consequences of the misalignment of the sleep-wake cycle with the biological night (Ingram, 2020). Circadian variability affects wakefulness, feeding behavior, metabolic function, and mood differently (Parkar et al., 2019; Poggiogalle et al., 2018; Zaki et al., 2018).
People have been divided into chronotype groups since the beginning of the 20th century (Becker et al., 2016). Chronotypes can generally be categorized into three types: Morning types, evening types, and non-types, which differ according to several behavioral, psychological, and biological variables, including usual eating times, appetite, mood, performance, and alertness (Kim & Kim, 2019; Kivelä et al., 2018). Morning types start their activities earlier in the morning, while evening types are more efficient later in the day (Matchock & Mordkoff, 2009). Morning types are tested in the morning, and evening types are tested in the evening. They respond more quickly to tasks that measure their reaction time (Lara et al., 2014). Shift workers usually undergo circadian misalignment, which appears when the feeding and sleep-wake cycles are desynchronized with the temporal framework organized by the internal biological clock. People differ considerably in their tolerance to shift work depending on their chronotype. Several studies have highlighted that evening types are a risk factor for depressive symptoms and the onset of depressive disorder in young people (Lotti et al., 2021). In studies that investigated the relationship between chronotype in university students, detrimental effects of sleep deprivation due to studying included decreased cognitive performance, lower motivation, increased aggression, increased depression, daytime sleepiness, and addictive behaviors (Montaruli et al., 2019; Van den Berg et al., 2018). Nursing and medical studies are also related to making up for sleep deprivation, circadian disruption, and missed weekend sleep on weekends or days off (López‐Soto et al., 2019; Sun et al., 2019).
It has been demonstrated that the circadian misalignment affects essential systems in the body. The link between misalignment of circadian rhythms, neurocognitive dysfunction, and substance use disorder may lie in the changed function of neural circuits underlying cognitive processing, reward, and impulse control (Hasler et al., 2015; Mattis & Sehgal, 2016; Wallace, 2020). Transgenic animal models show that circadian genes (e.g. Per1, Per2, and CLOCK) in reward circuits of the brain play a role in the regulation of appetitive behavior, and both clinical and preclinical research suggests a relationship between circadian genes and reward function (Rijo-Ferreira & Takahashi, 2019). Substantial neuroimaging literature has examined the possible links between circadian rhythm shifts and alterations in neural circuitry in the human brain (DePoy et al., 2017).
Given the increasingly stressful and heavy workload of the COVID-19 pandemic, circadian disorders and resulting complications are expected to increase in some health professionals and students (Marvaldi et al., 2021). It is essential for health policymakers to constantly update their information on the health status of health professionals and its changes over time to enable accurate and timely management. Considering that there are few epidemiological studies investigating circadian disorders in medical students, the present research was conducted to fill the gap in this critical point. The current study aimed to obtain information about circadian disorders and chronotype (as a mediating variable) on resulting mental states such as impulsivity, depression, anxiety, stress, addiction potential, and boredom in students of a medical university in northeastern Iran.
2. Materials and Methods
Study design and procedures
This research is a double-blind, randomized, controlled clinical trial. An overview of the study is provided in Figure 1. After written informed consent was obtained, an assistant randomly assigned subjects to the intervention or control group, and baseline data were obtained. Participants were asked to repeat the examinations at the end of the week.
Study participants
The intervention and control groups, selected from all students of Shahroud University of Medical Sciences, Shahroud City, Iran, were transferred to the experimental site in a specific dormitory for 11 days and housed in unique rooms where the light intensity is specially designed according to luxury, period and light reception time, hours of food intake. The inclusion criteria were male gender, right-handed, aged between 18 and 25 years, and regular sleep and wake rhythm in the last month (8 to 10 hours of sleep per night). The exclusion criteria were a past medical history of psychiatric illness, history of substance use, use of psychotropic drugs, a general medical disorder that endangers the subject’s health during the test, a history of brain trauma, metal bodies in the body, including platinum, fragments, or iron fragments, an irregular sleep and wake rhythm in the past month (8 to 10 hours of sleep per night), and a body mass index (BMI) greater than 30.
Randomization and blinding
To ensure the blinding of the investigators, the research coordinator carried out block randomization. Both participants and investigators are blinded to the group protocol. Participants were asked not to disclose details about their condition to their investigator to prevent unblinding. If subjects disclose their treatment, the investigator is immediately replaced by the blinded principal investigator of the project participant.
Study instruments
Reduced morningness-eveningness-questionnaire (rMEQ)
The German version of the rMEQ was applied to collect data. The rMEQ is a brief form of the morningness-eveningness questionnaire designed by Horne & Östberg, (1976). The original version contained 19 items and was rated on a Likert-type scale (Horne & Östberg, 1976). Adan & Almirall, (1991) identified a short version of this original form, which was then used in different countries, such as Iran (Adan & Almirall, 1991). rMEQ has adequate psychometric properties, good convergent and construct validity, and test re-test reliability. The scale contains 5 items linked to peak performance, preferred bedtime, time of rising, morning fatigue, and a global self-evaluation item. The Cronbach α was 0.62, and the German version was a reliable and valid measure of chronotype. Participants are classified with scores from high to low into the following types: A total rMEQ score of 18 and above as morning types, between 12 and 17 as intermediate types, and 11 and below as evening types (Adan & Almirall, 1991; Marvaldi et al., 2021).
Multidimensional state boredom scale (MSBS)
Fahlman et al., (2013) developed a MSBS as the first and full-scale measurement of state boredom (Fahlman et al., 2013). In the present study, we applied the Persian version of the MSBS, which was validated on a sample of adults by Mohseni-Ezhiyeh et al. (2017). It has a factor structure similar to the original questionnaire (i.e. 5 factors and 29 items). The Persian version of the MSBS is equivalent to the original version in terms of conceptual and linguistic features. The internal consistency of the Persian version of the MSBS was good. Its Cronbach α is 0.94 for the total score and between 0.80 and 0.89 for the subscale scores (Mohseni-Ezhiyeh & Ghamarani, 2017).
Addiction potential scale (APS)
Weed and Butcher created the APS in 1992 (Weed et al., 1992). In the current study, we used the Persian version of this scale designed by Zargar (2007). This scale contained 2 factors, 36 items, and 5 lie detector items. Most items of the first factor (the active factor) are associated with a tendency to substance use, depression, antisocial behavior, positive attitude to substance use, and sensation seeking. Most items of the second factor (the passive factor) are associated with a lack of depression and assertiveness. The criterion validity test revealed that the mentioned scale can discriminate well between substance users and non-users. The internal validity of this scale was 0.88 (Zargar et al., 2008).
Depression, anxiety, and stress scale-21 (DASS-21)
This study used data from 21 items of the depression, anxiety, and stress scale-42 (DASS-42) (i.e. the DASS-21) developed by Guillemin et al. (1993). Each of the three scales of the DASS-21 contains seven items. The items of the DASS-21 refer to the past week. Each item is scored on a 4-point Likert scale from 0 to 21. The higher the score indicated, the more severe the depression, anxiety, and stress (Asghari et al., 2008; Guillemin et al., 1993).
Barratt impulsiveness-11 (BIS-11)
The BIS-11 (11th version) was developed by Patton et al. (1995). It contains 30 items rated on a 5-point Likert scale. Twelve items are reverse-scored. It also includes three second-order parameters: Attention, motor skills, and non-planning. High scores indicate lower levels of attention, hyperactivity, and lack of planning. Its effectiveness in assessing impulsive dimensions is well established. In Iran, the norm is reduced to 25. In the present study, a 25-question form was used. The internal consistency of Persian BIS-11 is reported to be very acceptable (α=0.81) (Javid et al., 2012; Stanford et al., 2009).
Study intervention
Each participant underwent an 8-day study protocol to measure the effects of circadian misalignment on outcomes (Figure 2). One protocol applied circadian misalignment, and the other presented circadian alignment (Circadian alignment protocol, n=17; circadian misalignment protocol, n=18). On the first day of the 8-day study protocol, the subjects were accepted to the designated dormitory at ~8 AM to perform either the circadian rhythm alignment protocol or the circadian rhythm misalignment protocol (Figure 2). In the circadian alignment protocol, the subjects slept between 11:00 PM and 7:00 AM on days 1-8. In the circadian misalignment protocol, the subjects slept between 11:00 PM and 7:00 AM on days 1-3. On day 4 of the misalignment protocol, the subjects’ activation patterns were shifted by 12 hours, and this reversed cycle remained until the protocol’s end (day 8). The 12-hour shift on day 4 was made by an 8-hour wake episode and a 4-hour sleep opportunity, and the ratio of sleep opportunity to wake (1:2) remained the same in the adaptation and circadian alignment and misalignment protocols. Figure 2 shows the right conditions during the protocols.
Study outcomes
The outcome of this study is the change from baseline in scales measured by MSBS, APS, DASS-21, and BIS -11 by the end of the intervention.
Statistical analysis
Sample size calculation
The required sample size, according to Z(1-α)=1.96, power=0.9, α=0.05, d=0.8, and considering the rate of loss of 10% was calculated 34 (17 people in each group). Sample size was measured using the formula for randomized controlled trial studies as follows:
Efficacy analysis
All analyses were conducted in SPSS software, version 25. The two study groups’ pre-test and post-test Mean±SD were calculated. In preliminary analyses, we examined the pre-test result in two groups using the independent t-test (equality of means) and Levene’s test (equality of variances). We tested primary hypotheses regarding circadian misalignment effects on post-test measures using multivariate analysis of covariance (MANCOVA), Eta squared (η2), and power. We also categorized participants based on chronotype as a mediate variable within each group (circadian aligned and misaligned condition) to analyze outcomes using a one-way analysis of variance (ANOVA). We provide adjusted P to account for multiple comparisons of primary analyses using a Bonferroni post hoc test. The significance level was set at 0.05.
3. Results
Thirty-five participants were randomly assigned to circadian alignment/misalignment protocols (circadian alignment protocol, n=17; circadian misalignment protocol, n=18).
The mean age was 21.66 years (18-25 years). Thus, complete follow-up was available for 35 subjects. Figure 3 shows a consolidated standards of reporting trials (CONSORT) flowchart for the study. The obtained F value for the pre-test scores showed no significant difference between the groups at the pre-test (P>0.05).
As shown in Table 1, there is a difference between the mean scores of some research variables in the two measurement phases. Box’s test of equality of covariance matrices shows that the homogeneity of the variance-covariance matrix is satisfied (Box’s M=129.73, F=1.25, df=28, P=0.087).
The result of Wilks’ lambda test in the post-test showed that the independent variable (circadian misalignment) was effective on at least one of the dependent variables in the intervention group (F=5.88, df=13.8, P=0.009, ƞ2=0.90, 1-β=0.95). Analysis of covariance was used to evaluate the effect (Table 2).
Table 2 shows that circadian misalignment was effective in motor impulsivity, passive addiction potential, low arousal, inattention, and time perception. Results of the eta-squared coefficient show that the effect of circadian misalignment on motor impulsivity, passive addiction, low arousal, inattention, and time perception was high and that among the variables, the impact on time perception was the largest.
Table 3 presents a one-way ANOVA to compare research variables in groups based on chronotype (evening, intermediate, and morning types). There is a significant difference between the three groups of chronotype regarding total and non-planning impulsivity, as well as active and passive addiction potential.
The results of the Bonferroni post hoc test to compare the mean of variables in the chronotype groups about total and non-planning impulsivity scores, active and passive addiction showed that non-planning and active addiction in persons with evening and intermediate types were significantly lower than persons with morning type. The total scores of impulsivity and passive factors of addiction potential in participants with the morning type are significantly higher than in participants with the evening type. Table 4 presents the results of the Bonferroni post hoc test.
4. Discussion
In the present study, we aimed to investigate a one-week circadian misalignment resulting from an inversion of the activation cycle (such as the feeding and sleep-wake), which is typical in shift workers and medical students based on chronotype as a mediating variable, on impulsivity, depression, anxiety, stress, addiction potential, and boredom. The major findings from the present study are as follows. First, there was a significant association between circadian misalignment and motor impulsivity, passive factors of addiction potential, low arousal, inattention, and time perception (subscales of boredom). Second, persons with circadian misalignment and a morning type showed significantly more total and non-planning impulsivity and active and passive addiction potential in comparison with other types. The outcomes of this study have important hints for health care providers. Monitoring and paying attention to the mental health of medical care providers improves the quality of health services in the community.
In accordance with the relevant literature, our results indicate that participants involved in circadian misalignment have psychological conditions compared to a healthy control group with circadian-aligned conditions (Baron & Reid, 2014; Walker et al, 2020). Our findings showed that the problems comprised impulsivity, addiction potential, and boredom. Previous studies have shown that eveningness is a risk factor for impulsivity. Another consistent finding was that having an evening-type and circadian misalignment significantly related to impulsivity and addiction potential (Hwang et al., 2016; Kang et al., 2015; Selvi et al., 2011). In a systematic review, Gillett et al. (2021) reported a significant relationship between circadian rest-activity pattern disturbance (actigraphic variables) and impulsivity and mood disorder in participants aged 12–65. Also, our results, in line with the medical literature, showed circadian misalignment prospectively related to the potential of substance use (Claudatos et al., 2019; Logan et al., 2018). It is understood that impulsiveness makes a person prone to addiction. Tamura et al. reviewed the bidirectional relationship between substance use and the circadian system. They showed each drug follows a circadian pattern and changes during the development of substance use disorder. Furthermore, the expression of the CLOCK gene is also altered with the progression of addiction in many brain regions associated with reward circuits, addictive behaviors, and relapse (Tamura et al., 2021).
Multiple types of the research reported emotions, affect, mood, motivation, especially achievement emotions (e.g. boredom and anger), have been addressed in relation to chronotype (Fabbian et al., 2016; Itzek-Greulich, Randler, & Vollmer, 2016; Kadzikowska-Wrzosek, 2020). However, no study examined the effect of circadian misalignment on boredom. The present study showed a significant relationship between circadian misalignment and boredom. On the other hand, many preclinical and clinical studies have addressed a clear link between altered circadian system on depression, anxiety and stress, which was inconsistent with our findings (Blume et al., 2019; Difrancesco et al., 2019; Kim et al., 2017; Koch et al., 2017; Landgraf et al., 2016). Chellappa et al. conducted a study in 2020. They found circadian misalignment due to simulated night shifts significantly reduced mood and well-being levels throughout days of misalignment compared to circadian alignment conditions in the non-shift workers’ group (Chellappa et al., 2020). Several research studies have shown a potential causal relationship between disturbed circadian and hypothalamic-pituitary-adrenal axis dysregulation (Nader, Chrousos, & Kino, 2010). Also, animal models show that the circadian genes Per1 and Peir2 in the nucleus accumbens regulate anxiety-related behavior (Spencer et al., 2013). One possible explanation for inconsistent findings is our small sample size.
First, the sample size was small in terms of the study limitations. Second, neuropsychological variables were measured by self-report rather than behavioral and physiological measures via actigraphy. Third, the intervention protocol in this study was the same in all three groups: Morning types, intermediate types, and evening types. On the other hand, in this study, the researchers could not find a valid protocol that could be used separately for each of these three groups. Fourth, although we could recruit female participants due to cultural constraints, it could have led to serious and time-consuming problems in implementing this project. Future researchers are recommended to repeat the present study with female participants because there are significant differences in chronotype according to gender. It is also recommended that the study be conducted using different protocols based on different chronotypes to control the testing conditions better. Our findings add to previous literature by investigating the effectiveness of the circadian system on neuropsychiatric conditions. The results of this study have important implications for clinical care providers in terms of shift work.
5. Conclusion
Alterations in diurnal profiles of activity, sleep, and feeding time, based on chronotype related to impulsiveness and boredom, and such circadian misalignment is associated with addiction potential.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Review Committee of Shahroud University of Medical Sciences, Shahroud, Iran (Code: IR.SHMU.REC.1399.170). The study was designed and carried out based on the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research established by the Iranian Registry of Clinical Trials (IRCT), Tehran, Iran (Code: 20210202050223N1). All the participants signed their informed written consent.
Funding
The present study was extracted from the PhD dissertation of Mohammad Niroumand Sarvandani, approved by the Department of Addiction Studies, School of Medicine, Shahroud University of Medical Sciences, Shahroud, Iran (No.: 838). This study was financially supported by the Research Deputy of Shahroud University of Medical Sciences, Shahroud, Iran (Grant No.: 99119).
Authors' contributions
Conceptualization: Mohammad Niroumand Sarvandani; Methodology: Raheleh Rafaiee, Hamed Ghazvini and Behzad Garmabi; Formal analysis and software: Masoud Asadi; Investigation: Mohammad Niroumand Sarvandani, and Hamed Ghazvini; Writing the original draft: Raheleh Rafaiee, and Mohammad Niroumand Sarvandani; Review and editing: Hamid Kalalian Moghaddam; Funding acquisition, resources, and supervision: Hamid Kalalian Moghaddam; Final approval: All authors.
Conflict of interest
All authors declared no conflict of interest.
Acknowledgments
The authors appreciate all the individuals who collaborated in the study.
References
Adan, A., & Almirall, H. (1991). Horne & Östberg morningness-eveningness questionnaire: A reduced scale. Personality and Individual Differences, 12(3), 241-253. [DOI:10.1016/0191-8869(91)90110-W]
Asghari, A., Saed, F., & Dibajnia, P. (2008). Psychometric properties of the Depression Anxiety Stress Scales-21 (DASS 21) in a non clinical Iranian sample. International Journal of Psychology, 2(2), 82-102. [Link]
Baron, K. G., & Reid, K. J. (2014). Circadian misalignment and health. International Review of Psychiatry (Abingdon, England), 26(2), 139–154. [DOI:10.3109/09540261.2014.911149] [PMID]
Becker, K., Steinberg, H., & Kluge, M. (2016). Emil Kraepelin’s concepts of the phenomenology and physiology of sleep: The first systematic description of chronotypes. Sleep Medicine Reviews, 27, 9-19. [DOI:10.1016/j.smrv.2015.06.001] [PMID]
Blume, C., Garbazza, C., & Spitschan, M. (2019). Effects of light on human circadian rhythms, sleep and mood. Somnologie, 23(3), 147-156. [DOI:10.1007/s11818-019-00215-x] [PMID]
Chellappa, S. L., Morris, C. J., & Scheer, F. A. J. L. (2020). Circadian misalignment increases mood vulnerability in simulated shift work. Scientific Reports, 10(1), 18614. [DOI:10.1038/s41598-020-75245-9] [PMID]
Claudatos, S., Baker, F. C., & Hasler, B. P. (2019). Relevance of sleep and circadian rhythms to adolescent substance use. Current Addiction Reports, 6(4), 504-513. [DOI:10.1007/s40429-019-00277-9]
DePoy, L. M., McClung, C. A., & Logan, R. W. (2017). Neural mechanisms of circadian regulation of natural and drug reward. Neural Plasticity, 2017, 5720842. [DOI:10.1155/2017/5720842] [PMID]
Difrancesco, S., Lamers, F., Riese, H., Merikangas, K. R., Beekman, A. T. F., & van Hemert, A. M., et al. (2019). Sleep, circadian rhythm, and physical activity patterns in depressive and anxiety disorders: A 2 week ambulatory assessment study. Depression and Anxiety, 36(10), 975-986. [DOI:10.1002/da.22949] [PMID]
Fabbian, F., Zucchi, B., De Giorgi, A., Tiseo, R., Boari, B., & Salmi, R., et al. (2016). Chronotype, gender and general health. Chronobiology International, 33(7), 863–882. [DOI:10.1080/07420528.2016.1176927] [PMID]
Fahlman, S. A., Mercer Lynn, K. B., Flora, D. B., & Eastwood, J. D. (2013). Development and validation of the multidimensional state boredom scale. Assessment, 20(1), 68-85. [DOI:10.1177/1073191111421303] [PMID]
Gillett, G., Watson, G., Saunders, K. E., & McGowan, N. M. (2021). Sleep and circadian rhythm actigraphy measures, mood instability and impulsivity: A systematic review. Journal of Psychiatric Research, 144, 66-79. [DOI:10.1016/j.jpsychires.2021.09.043] [PMID]
Guillemin, F., Bombardier, C., & Beaton, D. (1993). Cross cultural adaptation of health related quality of life measures: Literature review and proposed guidelines. Journal of Clinical Epidemiology, 46(12), 1417-1432. [DOI:10.1016/0895-4356(93)90142-N] [PMID]
Hasler, B. P., Soehner, A. M., & Clark, D. B. (2015). Sleep and circadian contributions to adolescent alcohol use disorder. Alcohol, 49(4), 377-387. [DOI:10.1016/j.alcohol.2014.06.010] [PMID]
Horne, J. A., & Östberg, O. (1976). A self assessment questionnaire to determine morningness-eveningness in human circadian rhythms. International Journal of Chronobiology, 4(2), 97-110. [Link]
Hower, I. M., Harper, S. A., & Buford, T. W. (2018). Circadian rhythms, exercise, and cardiovascular health. Journal of Circadian Rhythms, 16, 7. [DOI:10.5334/jcr.164] [PMID]
Hwang, J. Y., Kang, S. G., Gwak, A. R., Park, J., & Lee, Y. J. (2016). The associations of morningness-eveningness with anger and impulsivity in the general population. Chronobiology International, 33(2), 200-209. [DOI:10.3109/07420528.2015.1128947] [PMID]
Ingram, K. K. (2020). Circadian rhythm sleep wake disorders (CRSWDs): Linking circadian misalignment to adverse health outcomes. EBioMedicine, 62, 103142. [DOI:10.1016/j.ebiom.2020.103142] [PMID]
Itzek Greulich, H., Randler, C., & Vollmer, C. (2016). The interaction of chronotype and time of day in a science course: Adolescent evening types learn more and are more motivated in the afternoon. Learning and Individual Differences, 51, 189-198. [DOI:10.1016/j.lindif.2016.09.013]
Javid, M., Mohammadi, N., & Rahimi, C. H. (2012). [Psychometric properties of an Iranian version of the Barratt Impulsiveness Scale 11 (BIS 11) (Persian)]. Psychological Models and Methods, 2(8), 23-34. [Link]
Kadzikowska Wrzosek, R. (2020). Insufficient sleep among adolescents: The role of bedtime procrastination, chronotype and autonomous vs. controlled motivational regulations. Current Psychology, 39(3), 1031-1040. [DOI:10.1007/s12144-018-9825-7]
Kang, J. I., Park, C. I., Sohn, S. Y., Kim, H. W., Namkoong, K., & Kim, S. J. (2015). Circadian preference and trait impulsivity, sensation seeking and response inhibition in healthy young adults. Chronobiology International, 32(2), 235-241. [DOI:10.3109/07420528.2014.965313] [PMID]
Kim, J., Jang, S., Choe, H. K., Chung, S., Son, G. H., & Kim, K. (2017). Implications of circadian rhythm in dopamine and mood regulation. Molecules and Cells, 40(7), 450-456. [DOI:10.14348/molcells.2017.0065] [PMID]
Kim, S., & Kim, S. J. (2019). Assessment and understanding of chronotype. Sleep Medicine and Psychophysiology, 26(1), 5-15. [Link]
Kivelä, L., Papadopoulos, M. R., & Antypa, N. (2018). Chronotype and psychiatric disorders. Current Sleep Medicine Reports, 4(2), 94-103. [DOI:10.1007/s40675-018-0113-8] [PMID]
Koch, C. E., Leinweber, B., Drengberg, B. C., Blaum, C., & Oster, H. (2017). Interaction between circadian rhythms and stress. Neurobiology of Stress, 6, 57–67. [DOI:10.1016/j.ynstr.2016.09.001] [PMID]
Landgraf, D., Long, J. E., Proulx, C. D., Barandas, R., Malinow, R., & Welsh, D. K. (2016). Genetic disruption of circadian rhythms in the suprachiasmatic nucleus causes helplessness, behavioral despair, and anxiety like behavior in mice. Biological Psychiatry, 80(11), 827-835. [DOI:10.1016/j.biopsych.2016.03.1050] [PMID]
Lara, T., Madrid, J. A., & Correa, Á. (2014). The vigilance decrement in executive function is attenuated when individual chronotypes perform at their optimal time of day. Plos One, 9(2), e88820. [DOI:10.1371/journal.pone.0088820] [PMID]
Lewis, P., Oster, H., Korf, H. W., Foster, R. G., & Erren, T. C. (2020). Food as a circadian time cue-evidence from human studies. Nature Reviews Endocrinology, 16(4), 213-223. [DOI:10.1038/s41574-020-0318-z] [PMID]
Logan, R. W., Hasler, B. P., Forbes, E. E., Franzen, P. L., Torregrossa, M. M., & Huang, Y. H., et al. (2018). Impact of sleep and circadian rhythms on addiction vulnerability in adolescents. Biological Psychiatry, 83(12), 987-996. [DOI:10.1016/j.biopsych.2017.11.035]
López Soto, P. J., Fabbian, F., Cappadona, R., Zucchi, B., Manfredini, F., & García Arcos, A., et al. (2019). Chronotype, nursing activity, and gender: A systematic review. Journal of Advanced Nursing, 75(4), 734-748. [DOI:10.1111/jan.13876] [PMID]
Lotti, S., Pagliai, G., Colombini, B., Sofi, F., & Dinu, M. (2021). Chronotype differences in energy intake, cardiometabolic risk parameters, cancer, and depression: A systematic review with meta analysis of observational studies. Advances in Nutrition (Bethesda, Md.), 13(1), 269–281. [DOI:10.1093/advances/nmab115] [PMID]
Marvaldi, M., Mallet, J., Dubertret, C., Moro, M. R., & Guessoum, S. B. (2021). Anxiety, depression, trauma related, and sleep disorders among healthcare workers during the COVID 19 pandemic: A systematic review and meta analysis. Neuroscience and Biobehavioral Reviews, 126, 252–264. [DOI:10.1016/j.neubiorev.2021.03.024] [PMID]
Matchock, R. L., & Mordkoff, J. T. (2009). Chronotype and time of day influences on the alerting, orienting, and executive components of attention. Experimental Brain Research, 192(2), 189-198. [DOI:10.1007/s00221-008-1567-6] [PMID]
Mattis, J., & Sehgal, A. (2016). Circadian rhythms, sleep, and disorders of aging. Trends in Endocrinology & Metabolism, 27(4), 192-203. [DOI:10.1016/j.tem.2016.02.003] [PMID]
Mohseni Ezhiyeh, A., & Ghamarani, A. (2017). [Psychometric characteristics of the Persian version of the Multidimensional State Boredom Scale (MSBS PV) in mothers of children with autism spectrum disorder (Persian)]. Journal of Rafsanjan University of Medical Sciences, 15(9), 821-834. [Link]
Montaruli, A., Castelli, L., Galasso, L., Mulè, A., Bruno, E., & Esposito, F., et al. (2019). Effect of chronotype on academic achievement in a sample of Italian university students. Chronobiology International, 36(11), 1482-1495. [DOI:10.1080/07420528.2019.1652831] [PMID]
Moreno, J. P., Crowley, S. J., Alfano, C. A., Hannay, K. M., Thompson, D., & Baranowski, T. (2019). Potential circadian and circannual rhythm contributions to the obesity epidemic in elementary school age children. The International Journal of Behavioral Nutrition and Physical Activity, 16(1), 25. [DOI:10.1186/s12966-019-0784-7] [PMID]
Nader, N., Chrousos, G. P., & Kino, T. (2010). Interactions of the circadian CLOCK system and the HPA axis. Trends in Endocrinology & Metabolism, 21(5), 277-286. [DOI:10.1016/j.tem.2009.12.011] [PMID]
Parkar, S. G., Kalsbeek, A., & Cheeseman, J. F. (2019). Potential role for the gut microbiota in modulating host circadian rhythms and metabolic health. Microorganisms, 7(2), 41. [DOI:10.3390/microorganisms7020041] [PMID]
Patke, A., Young, M. W., & Axelrod, S. (2020). Molecular mechanisms and physiological importance of circadian rhythms. Nature Reviews Molecular Cell Biology, 21(2), 67-84. [DOI:10.1038/s41580-019-0179-2] [PMID]
Patton, J. H., Stanford, M. S., & Barratt, E. S. (1995). Factor structure of the Barratt Impulsiveness Scale. Journal of Clinical Psychology, 51(6), 768-774. [DOI:10.1002/1097-4679(199511)51:63.0.co;2-1] [PMID]
Poggiogalle, E., Jamshed, H., & Peterson, C. M. (2018). Circadian regulation of glucose, lipid, and energy metabolism in humans. Metabolism: Clinical and Experimental, 84, 11–27. [DOI:10.1016/j.metabol.2017.11.017] [PMID]
Rijo Ferreira, F., & Takahashi, J. S. (2019). Genomics of circadian rhythms in health and disease. Genome Medicine, 11(1), 82. [DOI:10.1186/s13073-019-0704-0] [PMID]
Rivkees, S. A. (2007). The development of circadian rhythms: From animals to humans. Sleep Medicine Clinics, 2(3), 331-341. [DOI:10.1016/j.jsmc.2007.05.010] [PMID]
Selvi, Y., Aydin, A., Atli, A., Boysan, M., Selvi, F., & Besiroglu, L. (2011). Chronotype differences in suicidal behavior and impulsivity among suicide attempters. Chronobiology International, 28(2), 170-175. [DOI:10.3109/07420528.2010.535938] [PMID]
Spencer, S., Falcon, E., Kumar, J., Krishnan, V., Mukherjee, S., & Birnbaum, S. G., et al. (2013). Circadian genes Period 1 and Period 2 in the nucleus accumbens regulate anxiety related behavior. The European Journal of Neuroscience, 37(2), 242-250. [DOI:10.1111/ejn.12010] [PMID]
Stanford, M. S., Mathias, C. W., Dougherty, D. M., Lake, S. L., Anderson, N. E., & Patton, J. H. (2009). Fifty years of the Barratt Impulsiveness Scale: An update and review. Personality and Individual Differences, 47(5), 385-395. [DOI:10.1016/j.paid.2009.04.008]
Sun, J., Chen, M., Cai, W., Wang, Z., Wu, S., & Sun, X., et al. (2019). Chronotype: Implications for sleep quality in medical students. Chronobiology International, 36(8), 1115-1123. [DOI:10.1080/07420528.2019.1619181] [PMID]
Tamura, E. K., Oliveira Silva, K. S., Ferreira Moraes, F. A., Marinho, E. A. V., & Guerrero Vargas, N. N. (2021). Circadian rhythms and substance use disorders: A bidirectional relationship. Pharmacology Biochemistry and Behavior, 201, 173105. [DOI:10.1016/j.pbb.2021.173105] [PMID]
Van den Berg, J. F., Kivelä, L., & Antypa, N. (2018). Chronotype and depressive symptoms in students: An investigation of possible mechanisms. Chronobiology International, 35(9), 1248-1261. [DOI:10.1080/07420528.2018.1470531] [PMID]
Walker, W. H., 2nd, Walton, J. C., DeVries, A. C., & Nelson, R. J. (2020). Circadian rhythm disruption and mental health. Translational Psychiatry, 10(1), 28. [DOI:10.1038/s41398-020-0694-0] [PMID]
Wallace, N. K. (2020). Circadian rhythms and brain metabolism across the lifespan [PhD dissertation]. Washington: Washington State University. [Link]
Weed, N. C., Butcher, J. N., McKenna, T., & Ben Porath, Y. S. (1992). New measures for assessing alcohol and drug abuse with the MMPI 2: The APS and AAS. Journal of Personality Assessment, 58(2), 389–404. [DOI:10.1207/s15327752jpa5802_15] [PMID]
West, A. C., Smith, L., Ray, D. W., Loudon, A. S. I., Brown, T. M., & Bechtold, D. A. (2017). Misalignment with the external light environment drives metabolic and cardiac dysfunction. Nature Communications, 8(1), 417. [DOI:10.1038/s41467-017-00462-2] [PMID]
Type of Study: Original |
Subject:
Cognitive Neuroscience
Received: 2022/06/29 | Accepted: 2022/08/28 | Published: 2025/03/18
Received: 2022/06/29 | Accepted: 2022/08/28 | Published: 2025/03/18
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
![]()
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
